

Prospective Comparison of QFT-GIT and T-SPOT.TB Assays for Diagnosis of Active Tuberculosis
- PMID: 29651163
- PMCID: PMC5897568
- DOI: 10.1038/s41598-018-24285-3
Prospective Comparison of QFT-GIT and T-SPOT.TB Assays for Diagnosis of Active Tuberculosis
Abstract
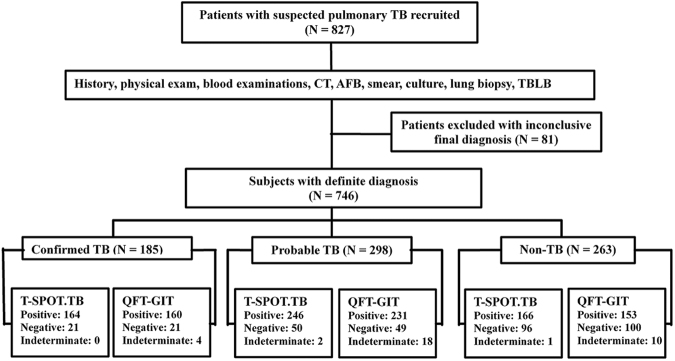
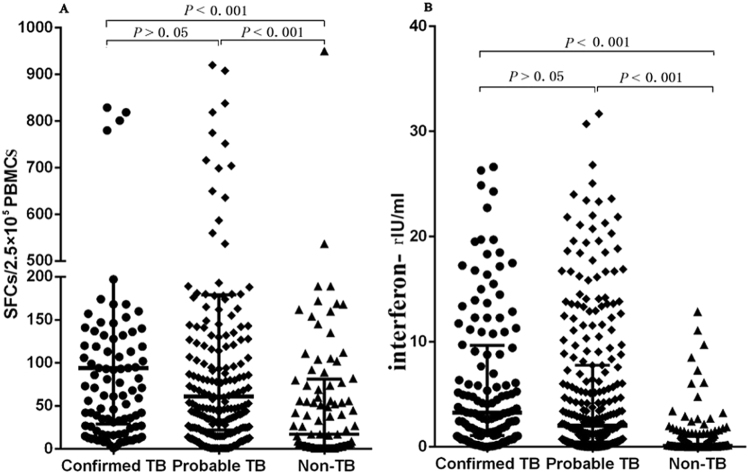
T-SPOT.TB and QuantiFERON-TB Gold In-Tube (QFT-GIT) tests, as two commercial blood assays for diagnosing active tuberculosis (ATB), are not yet fully validated. Especially, there are no reports on comparing the efficacy between the two tests in the same population in China. A multicenter, prospective comparison study was undertaken at four hospitals specializing in pulmonary diseases. A total of 746 suspected pulmonary TB were enrolled and categorized, including 185 confirmed TB, 298 probable TB and 263 non-TB. Of 32 patients with indeterminate test results (ITRs), age and underlying disease were associated with the rate of ITRs. Furthermore, the rate of ITRs determined by T-SPOT.TB was lower than QFT-GIT (0.4% vs. 4.3%, P < 0.01). When excluding ITRs, the sensitivities of T-SPOT.TB and QFT-GIT were 85.2% and 84.8%, and specificities of 63.4% and 60.5%, respectively in the diagnosis of ATB. The two assays have an overall agreement of 92.3%, but exhibited a poor linear correlation (r2 = 0.086) between the levels of interferon-γ release detected by the different assays. Although having some heterogeneity in detecting interferon-γ release, both the QFT-GIT and T-SPOT.TB demonstrated high concordance in diagnosing ATB. However, neither of them showed suitability in the definitive diagnosis of the disease.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- World Health Organization. Global tuberculosis control. 2016. Available at: http://www.who.int/tb/publications/global_report/en/ (2016).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
