

Epidemiology of sepsis in Brazil: Incidence, lethality, costs, and other indicators for Brazilian Unified Health System hospitalizations from 2006 to 2015
- PMID: 29652944
- PMCID: PMC5898754
- DOI: 10.1371/journal.pone.0195873
Epidemiology of sepsis in Brazil: Incidence, lethality, costs, and other indicators for Brazilian Unified Health System hospitalizations from 2006 to 2015
Abstract
Background: Sepsis is considered a major worldwide health burden, with high mortality and associated costs. Health indicators are essential to define strategies to improve the treatment of diseases, and the epidemiology information of sepsis in developing countries is scarce. Thus, the aim of this work is to assess trends in the incidence, lethality, costs, and other indicators of sepsis for Brazilian Unified Health System (SUS-Sistema Único de Saúde) hospitalizations for the period from January 2006 to December 2015.
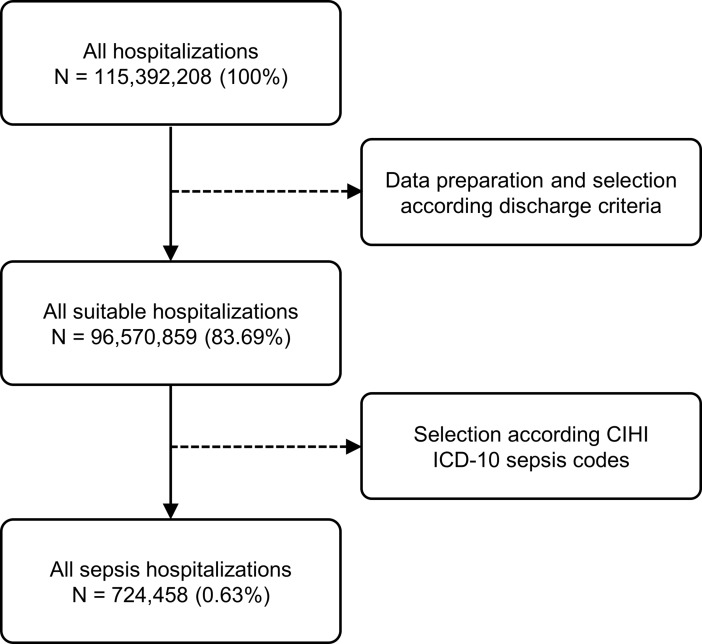
Materials and methods: We conducted this study using data from the SUS hospital information system. We selected registries of SUS hospitalizations of patients diagnosed with sepsis (total of 724,458 cases from 4,271 public and private Brazilian hospitals).
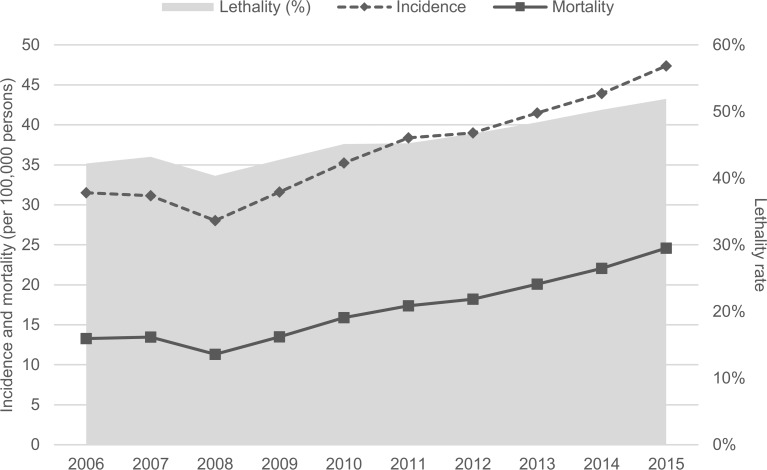
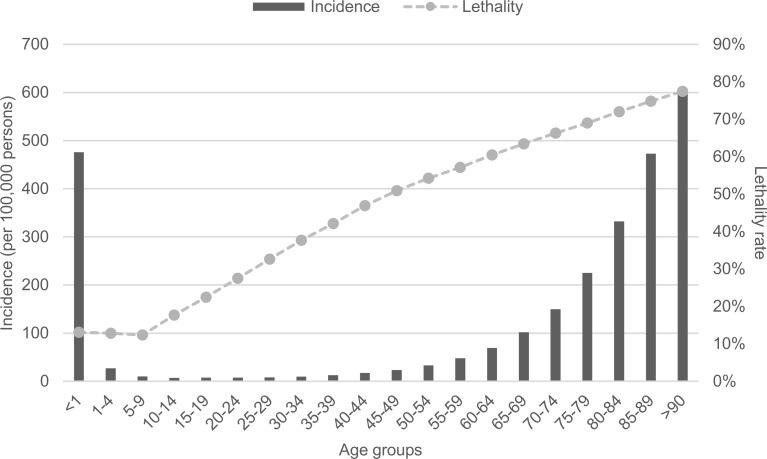
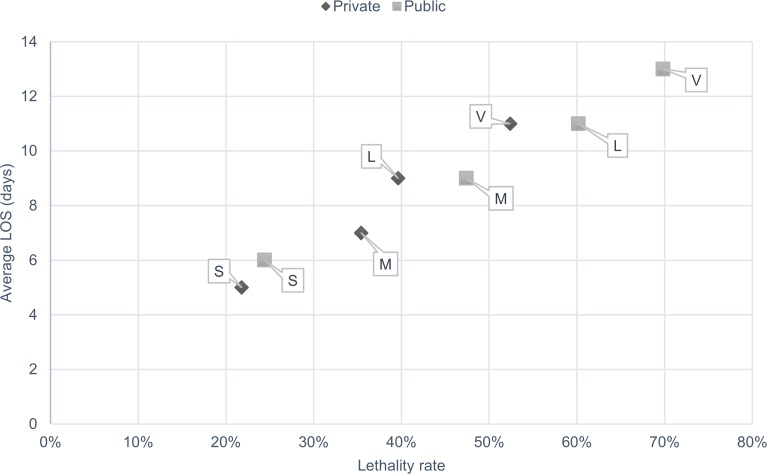
Results: From 2006 to 2015, the annual sepsis incidence increased 50.5% from 31.5/100,000 to 47.4/100,000 persons. The mean hospital length of stay (LOS) was 9.0 days. A total of 29.1% of the hospitalizations had admission to the intensive care unit (ICU) with a mean ICU LOS of 8.0 days. The mean cost per hospitalization was US$624.0 and for hospitalizations requiring intensive care was U$1,708.1. The overall sepsis lethality rate was 46.3%, and for hospitalizations with admission to the ICU, it was 64.5%. During the study period, the lethality rate for children/teenagers decreased 40.1%, but for all other age groups it increased 11.4%. The sepsis lethality rate in public hospitals (55.5%) was higher than private hospitals (37.0%) (p < 0.001). The mean hospitalization LOS for public hospitals (10.3 days) was higher than private hospitals (7.6 days) (p < 0.001).
Conclusions: The incidence and lethality rate of sepsis increased in SUS hospitalizations during the study period. The SUS's low reimbursement to hospitals for treating sepsis may be one of the reasons for the high lethality rate.
Conflict of interest statement
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315: 801–810. doi: 10.1001/jama.2016.0287 - DOI - PMC - PubMed
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States*. Crit Care Med. 2013;41: 1167–1174. doi: 10.1097/CCM.0b013e31827c09f8 - DOI - PubMed
-
- Kumar G, Kumar N, Taneja A, Kaleekal T, Tarima S, McGinley E, et al. Nationwide trends of severe sepsis in the 21st century (2000–2007). Chest. 2011;140: 1223–1231. doi: 10.1378/chest.11-0352 - DOI - PubMed
-
- Stoller J, Halpin L, Weis M, Aplin B, Qu W, Georgescu C, et al. Epidemiology of severe sepsis: 2008–2012. J Crit Care. 2016;31: 58–62. doi: 10.1016/j.jcrc.2015.09.034 - DOI - PubMed
-
- Kempker JA, Martin GS. The changing epidemiology and definitions of sepsis. Clin Chest Med. 2016;37: 165–179. doi: 10.1016/j.ccm.2016.01.002 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
