

NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease
- PMID: 29653606
- PMCID: PMC5958625
- DOI: 10.1016/j.jalz.2018.02.018
NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease
Abstract
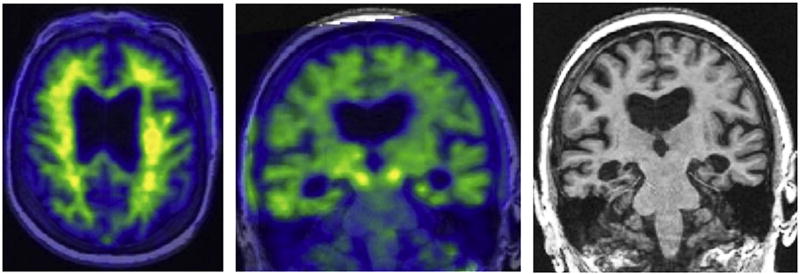
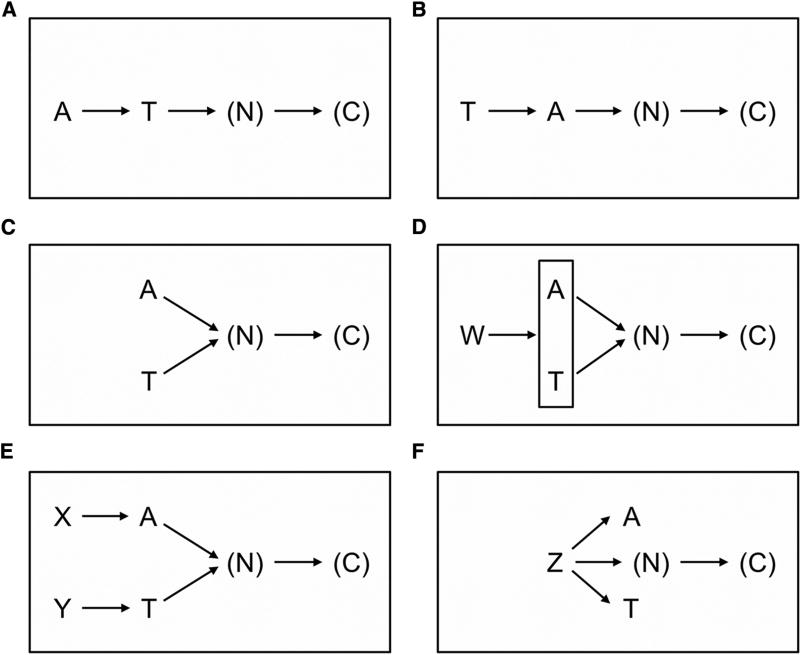
In 2011, the National Institute on Aging and Alzheimer's Association created separate diagnostic recommendations for the preclinical, mild cognitive impairment, and dementia stages of Alzheimer's disease. Scientific progress in the interim led to an initiative by the National Institute on Aging and Alzheimer's Association to update and unify the 2011 guidelines. This unifying update is labeled a "research framework" because its intended use is for observational and interventional research, not routine clinical care. In the National Institute on Aging and Alzheimer's Association Research Framework, Alzheimer's disease (AD) is defined by its underlying pathologic processes that can be documented by postmortem examination or in vivo by biomarkers. The diagnosis is not based on the clinical consequences of the disease (i.e., symptoms/signs) in this research framework, which shifts the definition of AD in living people from a syndromal to a biological construct. The research framework focuses on the diagnosis of AD with biomarkers in living persons. Biomarkers are grouped into those of β amyloid deposition, pathologic tau, and neurodegeneration [AT(N)]. This ATN classification system groups different biomarkers (imaging and biofluids) by the pathologic process each measures. The AT(N) system is flexible in that new biomarkers can be added to the three existing AT(N) groups, and new biomarker groups beyond AT(N) can be added when they become available. We focus on AD as a continuum, and cognitive staging may be accomplished using continuous measures. However, we also outline two different categorical cognitive schemes for staging the severity of cognitive impairment: a scheme using three traditional syndromal categories and a six-stage numeric scheme. It is important to stress that this framework seeks to create a common language with which investigators can generate and test hypotheses about the interactions among different pathologic processes (denoted by biomarkers) and cognitive symptoms. We appreciate the concern that this biomarker-based research framework has the potential to be misused. Therefore, we emphasize, first, it is premature and inappropriate to use this research framework in general medical practice. Second, this research framework should not be used to restrict alternative approaches to hypothesis testing that do not use biomarkers. There will be situations where biomarkers are not available or requiring them would be counterproductive to the specific research goals (discussed in more detail later in the document). Thus, biomarker-based research should not be considered a template for all research into age-related cognitive impairment and dementia; rather, it should be applied when it is fit for the purpose of the specific research goals of a study. Importantly, this framework should be examined in diverse populations. Although it is possible that β-amyloid plaques and neurofibrillary tau deposits are not causal in AD pathogenesis, it is these abnormal protein deposits that define AD as a unique neurodegenerative disease among different disorders that can lead to dementia. We envision that defining AD as a biological construct will enable a more accurate characterization and understanding of the sequence of events that lead to cognitive impairment that is associated with AD, as well as the multifactorial etiology of dementia. This approach also will enable a more precise approach to interventional trials where specific pathways can be targeted in the disease process and in the appropriate people.
Keywords: Alzheimer's disease diagnosis; Alzheimer's disease imaging; Amyloid PET; Biomarkers Alzheimer's disease; CSF biomarkers Alzheimer's disease; Preclinical Alzheimer's disease; Tau PET.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors’ conflict of interest statements can be viewed online at
Figures
Comment in
-
NIA commentary on the NIA-AA Research Framework: Towards a biological definition of Alzheimer's disease.Alzheimers Dement. 2018 Apr;14(4):576-578. doi: 10.1016/j.jalz.2018.03.004. Alzheimers Dement. 2018. PMID: 29653608 No abstract available.
References
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34:939–44. - PubMed
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Assocation workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:280–92. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
