

A Comparative Study of Carvedilol Versus Metoprolol Initiation and 1-Year Mortality Among Individuals Receiving Maintenance Hemodialysis
- PMID: 29653770
- PMCID: PMC6477681
- DOI: 10.1053/j.ajkd.2018.02.350
A Comparative Study of Carvedilol Versus Metoprolol Initiation and 1-Year Mortality Among Individuals Receiving Maintenance Hemodialysis
Abstract
Background: Carvedilol and metoprolol are the β-blockers most commonly prescribed to US hemodialysis patients, accounting for ∼80% of β-blocker prescriptions. Despite well-established pharmacologic and pharmacokinetic differences between the 2 medications, little is known about their relative safety and efficacy in the hemodialysis population.
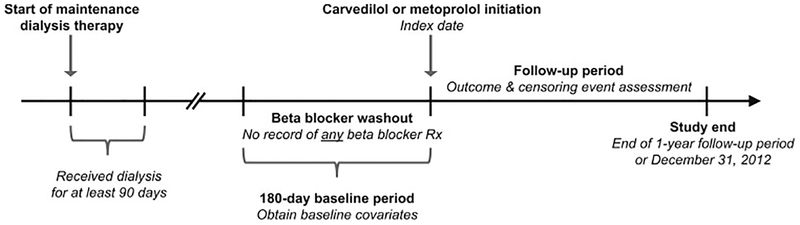
Study design: A retrospective cohort study using a new-user design.
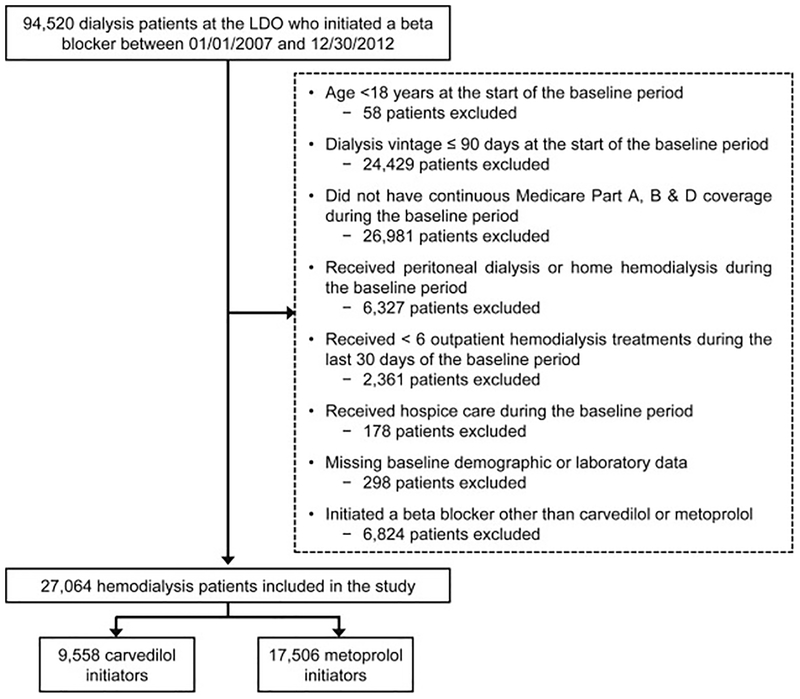
Setting & participants: Medicare-enrolled hemodialysis patients treated at a large US dialysis organization who initiated carvedilol or metoprolol therapy from January 1, 2007, through December 30, 2012.
Predictor: Carvedilol versus metoprolol initiation.
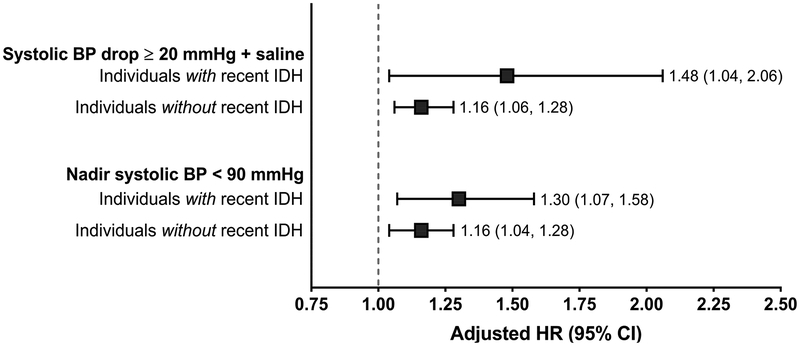
Outcomes: All-cause mortality, cardiovascular mortality, and intradialytic hypotension (systolic blood pressure decrease ≥ 20mmHg during hemodialysis plus intradialytic saline solution administration) during a 1-year follow-up period.
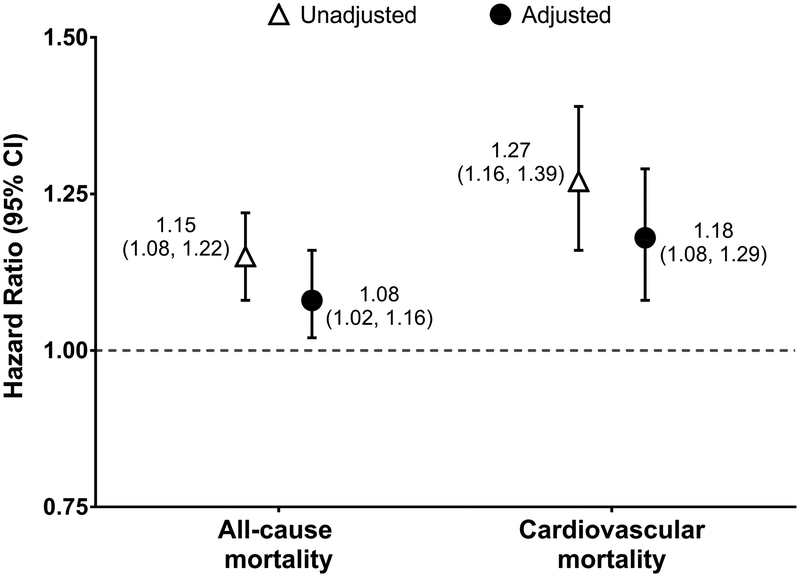
Measurements: Survival models were used to estimate HRs and 95% CIs in mortality analyses. Poisson regression was used to estimate incidence rate ratios (IRRs) and 95% CIs in intradialytic hypotension analyses. Inverse probability of treatment weighting was used to adjust for several demographic, clinical, laboratory, and dialysis treatment covariates in all analyses.
Results: 27,064 individuals receiving maintenance hemodialysis were included: 9,558 (35.3%) carvedilol initiators and 17,506 (64.7%) metoprolol initiators. Carvedilol (vs metoprolol) initiation was associated with greater all-cause (adjusted HR, 1.08; 95% CI, 1.02-1.16) and cardiovascular mortality (adjusted HR, 1.18; 95% CI, 1.08-1.29). In subgroup analyses, similar associations were observed among patients with hypertension, atrial fibrillation, heart failure, and a recent myocardial infarction, the main cardiovascular indications for β-blocker therapy. During follow-up, carvedilol (vs metoprolol) initiators had a higher rate of intradialytic hypotension (adjusted IRR, 1.10; 95% CI, 1.09-1.11).
Limitations: Residual confounding may exist.
Conclusions: Relative to metoprolol initiation, carvedilol initiation was associated with higher 1-year all-cause and cardiovascular mortality. One potential mechanism for these findings may be the increased occurrence of intradialytic hypotension after carvedilol (vs metoprolol) initiation.
Keywords: Beta-blocker; blood pressure; cardiovascular; carvedilol; dialyzability; end-stage renal disease (ESRD); hemodialysis; hypotension; intradialytic hypotension (IDH); metoprolol; mortality; pharmacoepidemiology.
Copyright © 2018 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Heterogeneity in Outcomes Among β-Blockers Elucidated by Intradialytic Data.Am J Kidney Dis. 2018 Sep;72(3):318-321. doi: 10.1053/j.ajkd.2018.03.032. Am J Kidney Dis. 2018. PMID: 30144835 No abstract available.
References
-
- Marengoni A, Onder G. Guidelines, polypharmacy, and drug-drug interactions in patients with multimorbidity. BMJ. 2015;350:h1059. - PubMed
-
- Coca SG, Krumholz HM, Garg AX, Parikh CR. Underrepresentation of renal disease in randomized controlled trials of cardiovascular disease. JAMA. 2006;296(11):1377–1384. - PubMed
-
- Konstantinidis I, Nadkarni GN, Yacoub R, et al. Representation of Patients With Kidney Disease in Trials of Cardiovascular Interventions: An Updated Systematic Review. JAMA Intern Med. 2016;176(1):121–124. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
