

Can microstructural MRI detect subclinical tissue injury in subjects with asymptomatic cervical spinal cord compression? A prospective cohort study
- PMID: 29654015
- PMCID: PMC5905727
- DOI: 10.1136/bmjopen-2017-019809
Can microstructural MRI detect subclinical tissue injury in subjects with asymptomatic cervical spinal cord compression? A prospective cohort study
Abstract
Objectives: Degenerative cervical myelopathy (DCM) involves extrinsic spinal cord compression causing tissue injury and neurological dysfunction. Asymptomatic spinal cord compression (ASCC) is more common, but its significance is poorly defined. This study investigates if: (1) ASCC can be automatically diagnosed using spinal cord shape analysis; (2) multiparametric quantitative MRI can detect similar spinal cord tissue injury as previously observed in DCM.
Design: Prospective observational longitudinal cohort study.
Setting: Single centre, tertiary care and research institution.
Participants: 40 neurologically intact subjects (19 female, 21 male) divided into groups with and without ASCC.
Interventions: None.
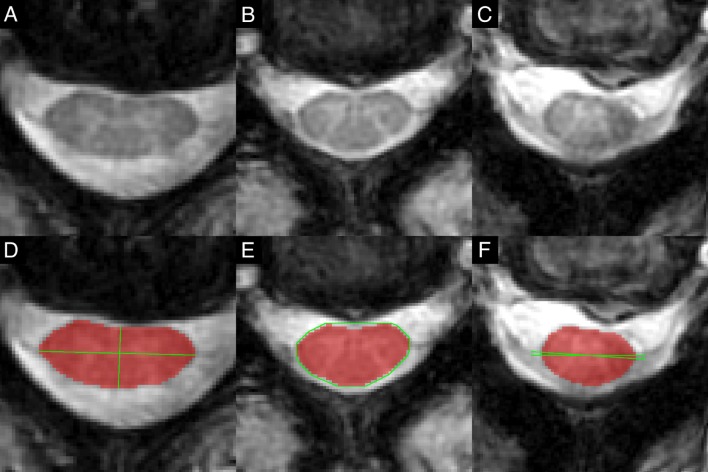
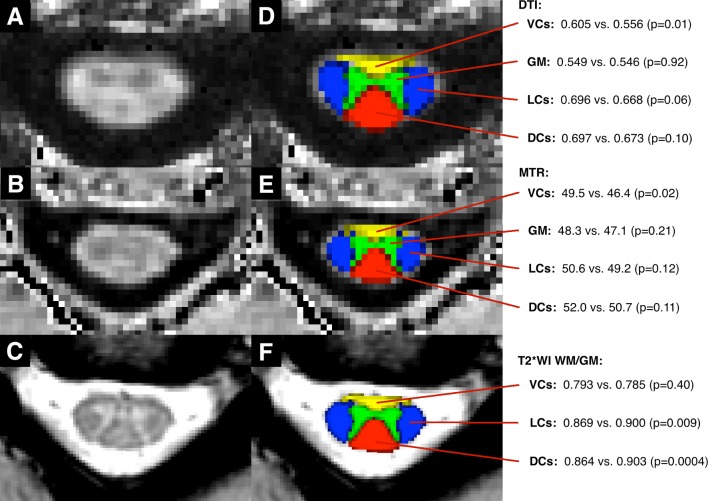
Outcome measures: Clinical assessments: modified Japanese Orthopaedic Association score and physical examination. 3T MRI assessments: automated morphometric analysis compared with consensus ratings of spinal cord compression, and measures of tissue injury: cross-sectional area, diffusion fractional anisotropy, magnetisation transfer ratio and T2*-weighted imaging white to grey matter signal intensity ratio (T2*WI WM/GM) extracted from rostral (C1-3), caudal (C6-7) and maximally compressed levels.
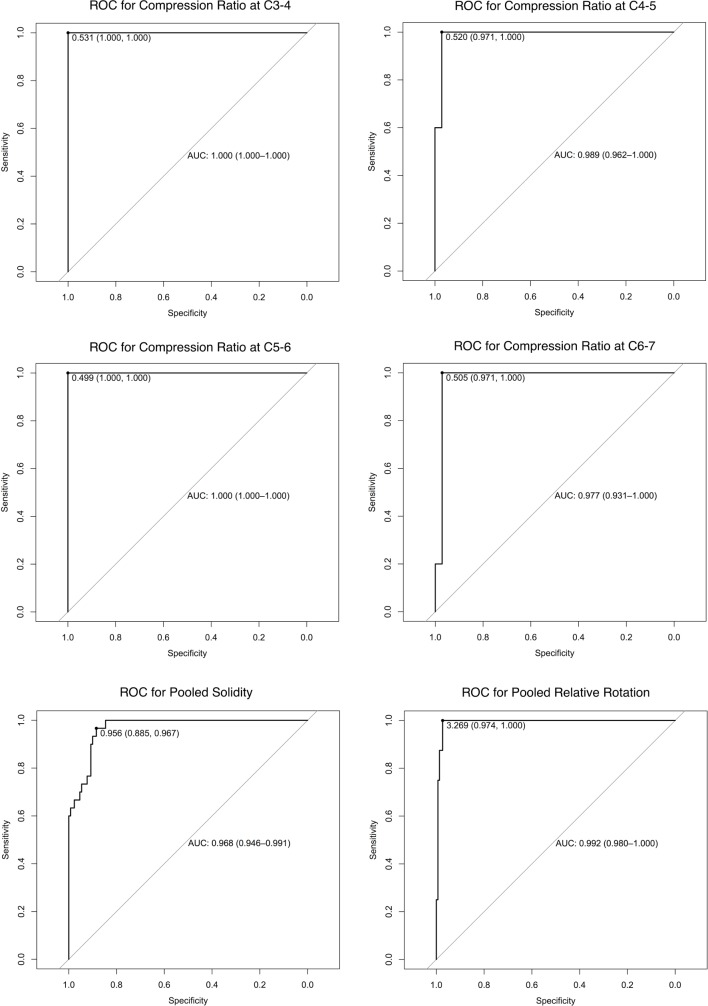
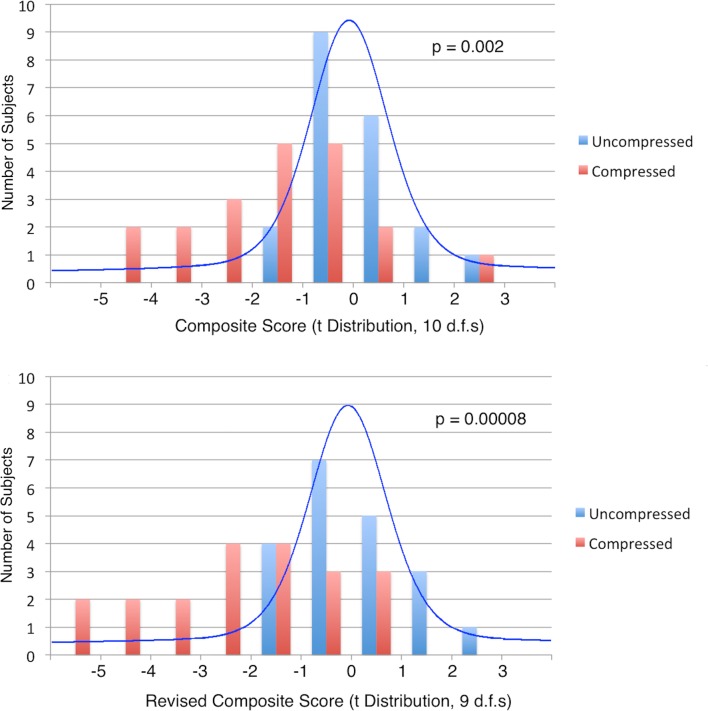
Results: ASCC was present in 20/40 subjects. Diagnosis with automated shape analysis showed area under the curve >97%. Five MRI metrics showed differences suggestive of tissue injury in ASCC compared with uncompressed subjects (p<0.05), while a composite of all 10 measures (average of z scores) showed highly significant differences (p=0.002). At follow-up (median 21 months), two ASCC subjects developed DCM.
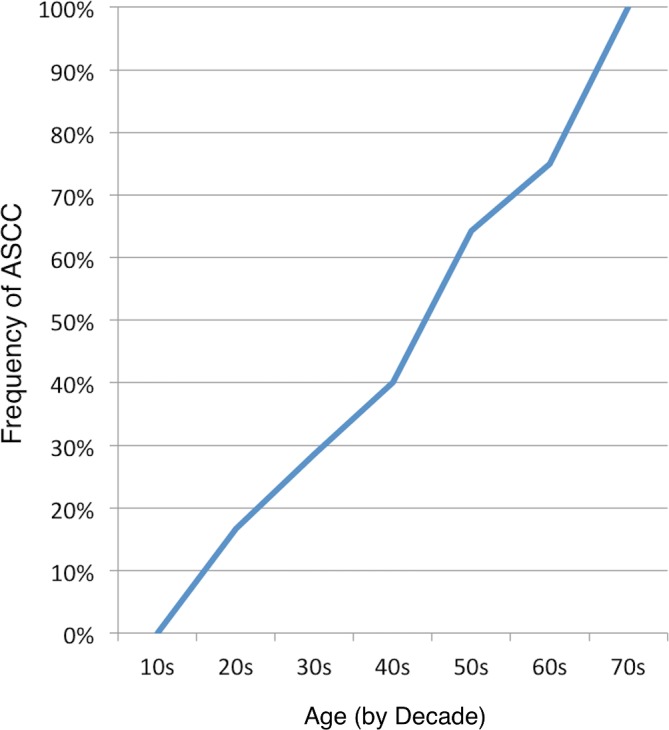
Conclusions: ASCC appears to be common and can be accurately and objectively diagnosed with automated morphometric analysis. Quantitative MRI appears to detect subclinical tissue injury in ASCC prior to the onset of neurological symptoms and signs. These findings require further validation, but offer the intriguing possibility of presymptomatic diagnosis and treatment of DCM and other spinal pathologies.
Keywords: diffusion tensor imaging; magnetization transfer; myelopathy; preclinical; quantitative mri; spinal cord injury.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical