

Assessing prevalence of missed laboratory-confirmed sexually transmitted infections among women in Kingston, Jamaica: results from a secondary analysis of the Sino-Implant clinical trial
- PMID: 29654017
- PMCID: PMC5905734
- DOI: 10.1136/bmjopen-2017-019913
Assessing prevalence of missed laboratory-confirmed sexually transmitted infections among women in Kingston, Jamaica: results from a secondary analysis of the Sino-Implant clinical trial
Abstract
Objectives: To assess potentially missed sexually transmitted infections (STIs), we compared clinically diagnosed STIs to laboratory-confirmed diagnoses of gonorrhoea (GC), chlamydia (CT) and trichomonas (Tvag).
Design: Secondary analysis of a randomised controlled trial.
Setting: We used data and specimens previously collected for the Sino-Implant Study in Kingston, Jamaica.
Participants: The Sino-Implant Study randomised 414 women to receive a levonorgestrel implant at either baseline or 3 months post-enrolment to evaluate unprotected sex after implant initiation. This analysis used 254 available vaginal swab samples.
Outcome measures: Clinically diagnosed STIs were determined from medical records by assessing clinical impressions and prescriptions. Laboratory-confirmed STIs included GC, CT and Tvag tested by Aptima Combo 2 for CT/GC and Aptima Tvag assays (Hologic, San Diego, California, USA). Log-binomial regression models fit with generalised estimating equations were used to estimate associations of clinically diagnosed STIs with laboratory-confirmed diagnoses and demographic and behavioural characteristics.
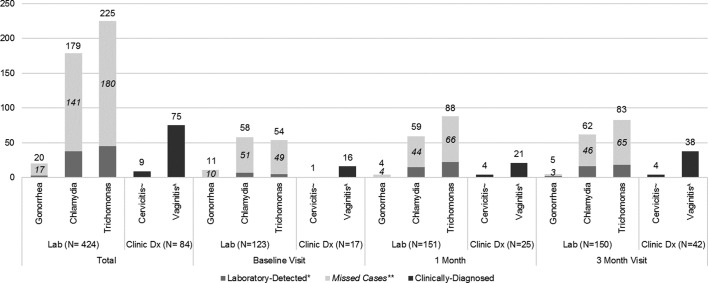
Results: Overall, 195 (76.8%) women had laboratory-confirmed STI (CT, GC or Tvag) while only 65 (25.6%) women had clinically diagnosed cervicitis and/or vaginitis during the study period. Clinical diagnosis missed 79.7% of laboratory-confirmed STIs: 85% of GC (n=17/20), 78.8% of CT (n=141/179) and 80.0% of Tvag (n=180/225). Hormonal contraceptive use in the month prior to the study visit was significantly associated with clinical diagnosis at any time point (prevalence ratio (PR): 1.65, 95% CI 1.07 to 2.54). As age increased, clinically missed infections significantly decreased (PR: 0.98 per year increase, 95% CI 0.97 to 1.00).
Conclusions: The prevalence of laboratory-confirmed STIs was much higher than what was captured by clinical diagnosis. GC, CT and Tvag were not accurately detected without lab confirmation. Missed diagnoses decreased with older age. Increased laboratory capacity and refinement of the syndromic approach are needed to protect the health of sexually active Jamaican women.
Trial registration number: NCT01684358.
Keywords: epidemiology; international health services; reproductive medicine.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Organization WH. Progress report of the implementation of the global strategy for prevention and control of sexually transmitted infections: 2006-2015. Geneva, Switzerland: World Health Organization, 2015.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous