

Dysregulation of serum bile acids and FGF19 in alcoholic hepatitis
- PMID: 29654817
- PMCID: PMC6054564
- DOI: 10.1016/j.jhep.2018.03.031
Dysregulation of serum bile acids and FGF19 in alcoholic hepatitis
Abstract
Background & aims: The degree of cholestasis is an important disease driver in alcoholic hepatitis, a severe clinical condition that needs new biomarkers and targeted therapies. We aimed to identify the largely unknown mechanisms and biomarkers linked to cholestasis in alcoholic hepatitis.
Methods: Herein, we analyzed a well characterized cohort of patients with alcoholic hepatitis and correlated clinical and histological parameters and outcomes with serum bile acids and fibroblast growth factor 19 (FGF19), a major regulator of bile acid synthesis.
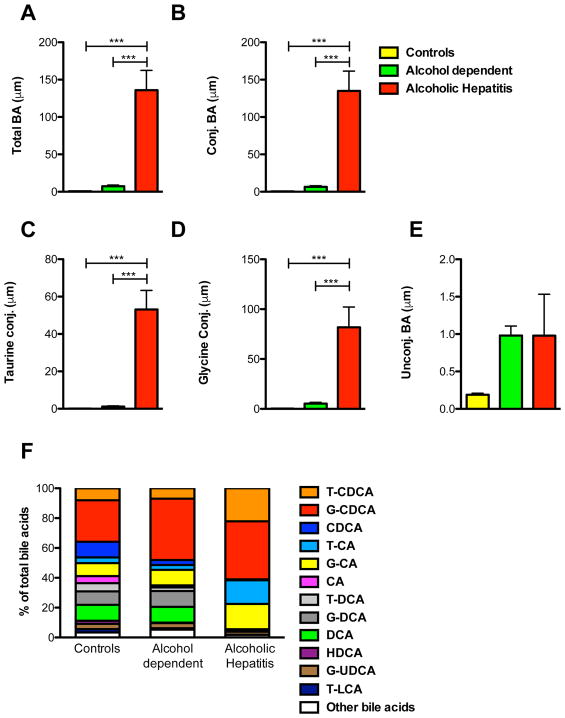
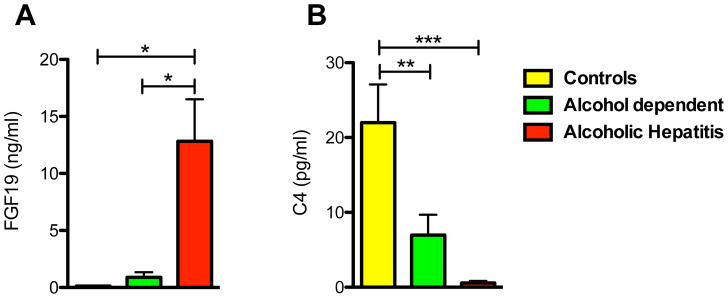
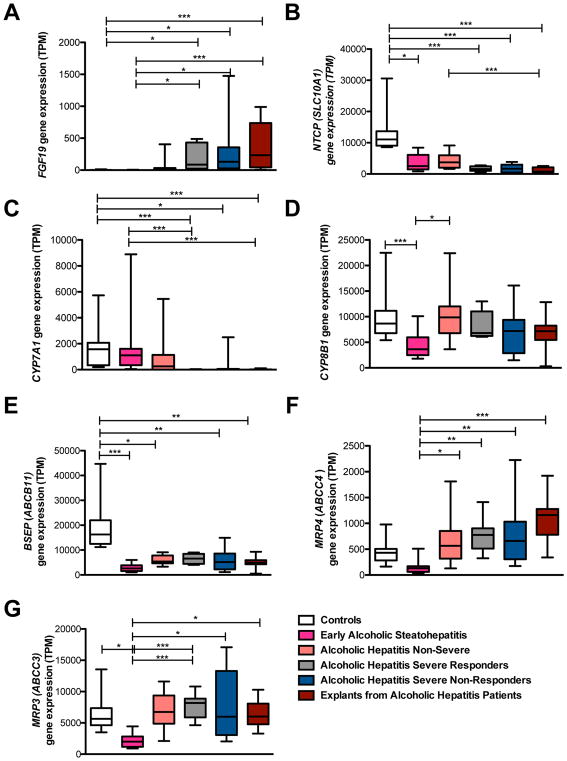
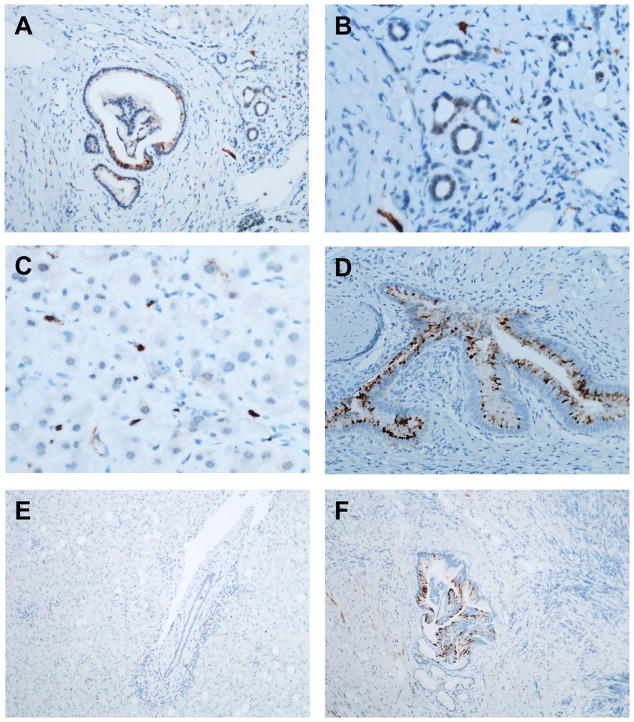
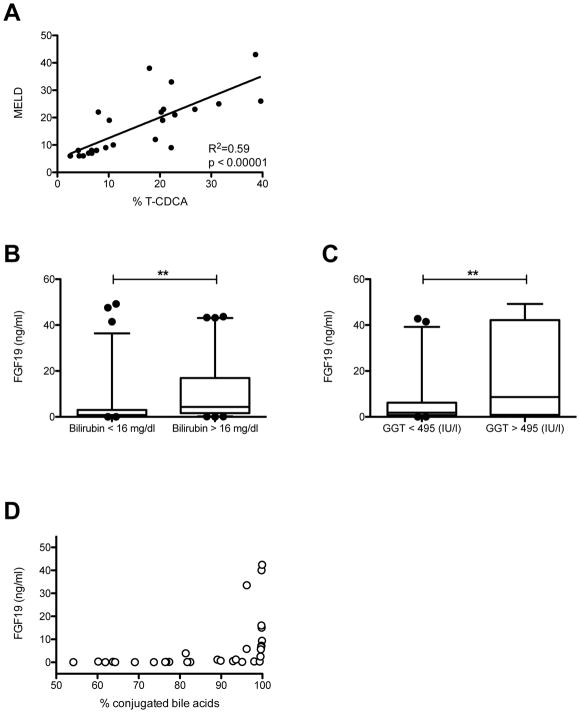
Results: We found that total and conjugated bile acids were significantly increased in patients with alcoholic hepatitis compared with controls. Serum FGF19 levels were strongly increased and gene expression of FGF19 was induced in biliary epithelial cells and ductular cells of patients with alcoholic hepatitis. De novo bile acid synthesis (CYP7A1 gene expression and C4 serum levels) was significantly decreased in patients with alcoholic hepatitis. Importantly, total and conjugated bile acids correlated positively with FGF19 and with disease severity (model for end-stage liver disease score). FGF19 correlated best with conjugated cholic acid, and model for end-stage liver disease score best with taurine-conjugated chenodeoxycholic acid. Univariate analysis demonstrated significant associations between FGF19 and bilirubin as well as gamma glutamyl transferase, and negative correlations between FGF19 and fibrosis stage as well as polymorphonuclear leukocyte infiltration, in all patients with alcoholic hepatitis.
Conclusion: Serum FGF19 and bile acids are significantly increased in patients with alcoholic hepatitis, while de novo bile acid synthesis is suppressed. Modulation of bile acid metabolism or signaling could represent a promising target for treatment of alcoholic hepatitis in humans.
Lay summary: Understanding the underlying mechanisms that drive alcoholic hepatitis is important for the development of new biomarkers and targeted therapies. Herein, we describe a molecule that is increased in patients with alcoholic hepatitis. Modulating the molecular pathway of this molecule might lead to promising targets for the treatment of alcoholic hepatitis.
Keywords: Bile acids; FGF19; Microbiome.
Published by Elsevier B.V.
Conflict of interest statement
Figures
Comment in
-
Exploring new treatment paradigms for alcoholic hepatitis by extrapolating from NASH and cholestasis.J Hepatol. 2018 Aug;69(2):275-277. doi: 10.1016/j.jhep.2018.05.012. Epub 2018 May 21. J Hepatol. 2018. PMID: 29792896 Free PMC article. No abstract available.
-
Finding fibroblast growth factor 19 during cholestasis: Does x mark the spot?J Hepatol. 2018 Dec;69(6):1399-1400. doi: 10.1016/j.jhep.2018.09.008. Epub 2018 Oct 4. J Hepatol. 2018. PMID: 30293670 No abstract available.
-
Reply to: "Finding fibroblast growth factor 19 during cholestasis: Does x mark the spot?J Hepatol. 2018 Dec;69(6):1400-1401. doi: 10.1016/j.jhep.2018.09.017. Epub 2018 Oct 6. J Hepatol. 2018. PMID: 30301625 No abstract available.
References
-
- Chacko KR, Reinus J. Spectrum of Alcoholic Liver Disease. Clin Liver Dis. 2016;20(3):419–427. - PubMed
-
- Thursz MR, Forrest EH, Ryder S investigators S. Prednisolone or Pentoxifylline for Alcoholic Hepatitis. N Engl J Med. 2015;373(3):282–283. - PubMed
-
- Maddrey WC, Boitnott JK, Bedine MS, Weber FL, Jr, Mezey E, White RI., Jr Corticosteroid therapy of alcoholic hepatitis. Gastroenterology. 1978;75(2):193–199. - PubMed
-
- Dominguez M, Rincon D, Abraldes JG, Miquel R, Colmenero J, Bellot P, et al. A new scoring system for prognostic stratification of patients with alcoholic hepatitis. Am J Gastroenterol. 2008;103(11):2747–2756. - PubMed
-
- Mathurin P, Lucey MR. Management of alcoholic hepatitis. J Hepatol. 2012;56(Suppl):S39–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
