

Wall stress on ascending thoracic aortic aneurysms with bicuspid compared with tricuspid aortic valve
- PMID: 29656820
- PMCID: PMC8447844
- DOI: 10.1016/j.jtcvs.2018.03.004
Wall stress on ascending thoracic aortic aneurysms with bicuspid compared with tricuspid aortic valve
Abstract
Objective: Guidelines for repair of bicuspid aortic valve-associated ascending thoracic aortic aneurysms have been changing, most recently to the same criteria as tricuspid aortic valve-ascending thoracic aortic aneurysms. Rupture/dissection occurs when wall stress exceeds wall strength. Recent studies suggest similar strength of bicuspid aortic valve versus tricuspid aortic valve-ascending thoracic aortic aneurysms; thus, comparative wall stress may better predict dissection in bicuspid aortic valve versus tricuspid aortic valve-ascending thoracic aortic aneurysms. Our aim was to determine whether bicuspid aortic valve-ascending thoracic aortic aneurysms had higher wall stresses than their tricuspid aortic valve counterparts.
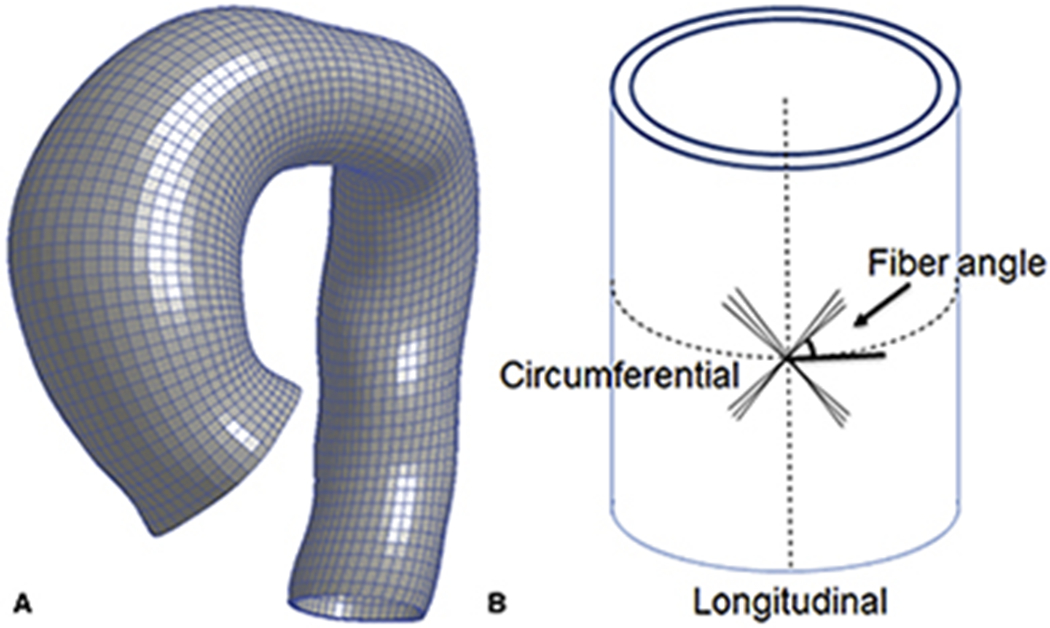
Methods: Patients with bicuspid aortic valve- and tricuspid aortic valve-ascending thoracic aortic aneurysms (bicuspid aortic valve = 17, tricuspid aortic valve = 19) greater than 4.5 cm underwent electrocardiogram-gated computed tomography angiography. Patient-specific 3-dimensional geometry was reconstructed and loaded to systemic pressure after accounting for prestress geometry. Finite element analyses were performed using the LS-DYNA solver (LSTC Inc, Livermore, Calif) with user-defined fiber-embedded material model to determine ascending thoracic aortic aneurysm wall stress.
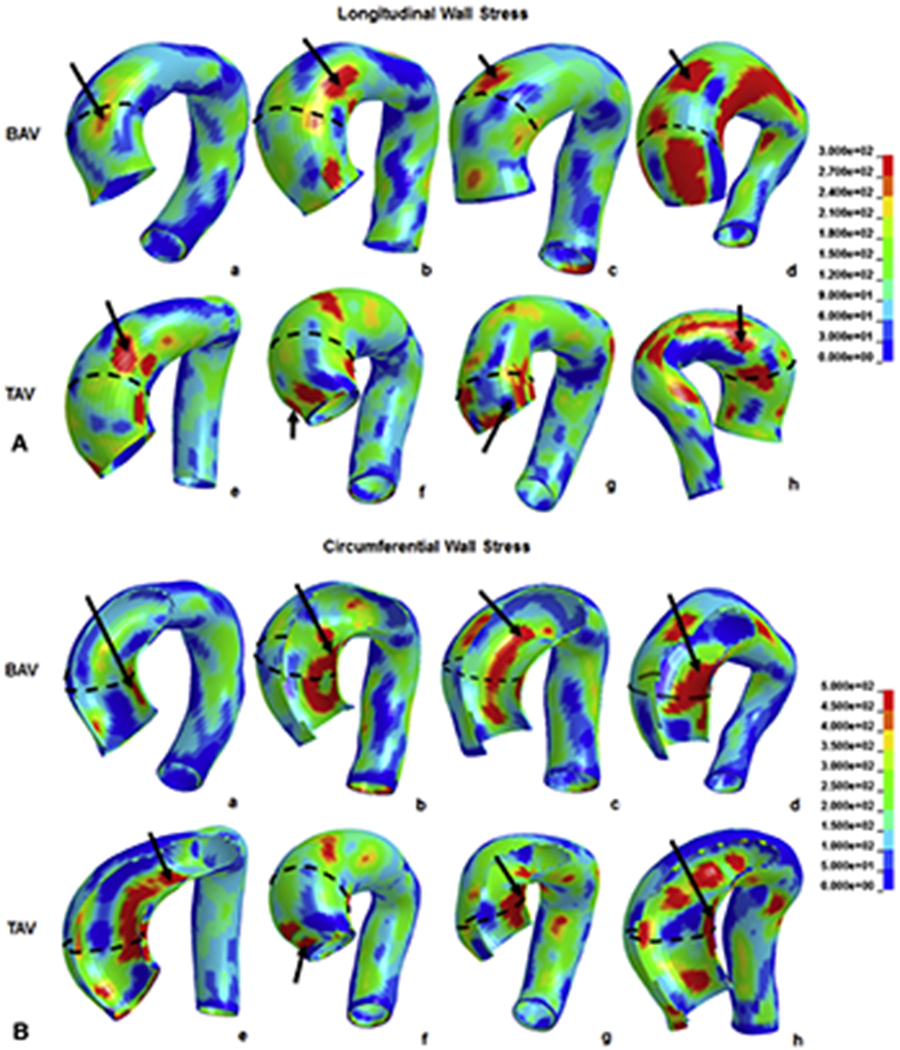
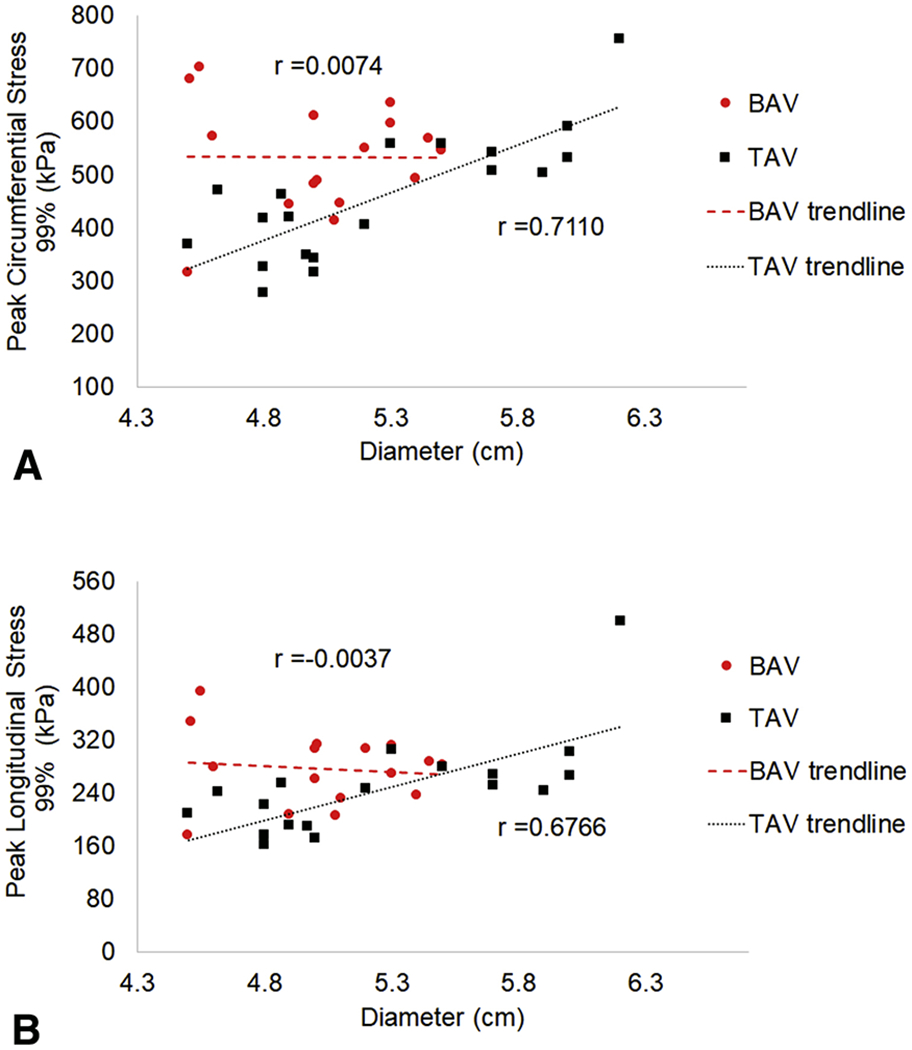
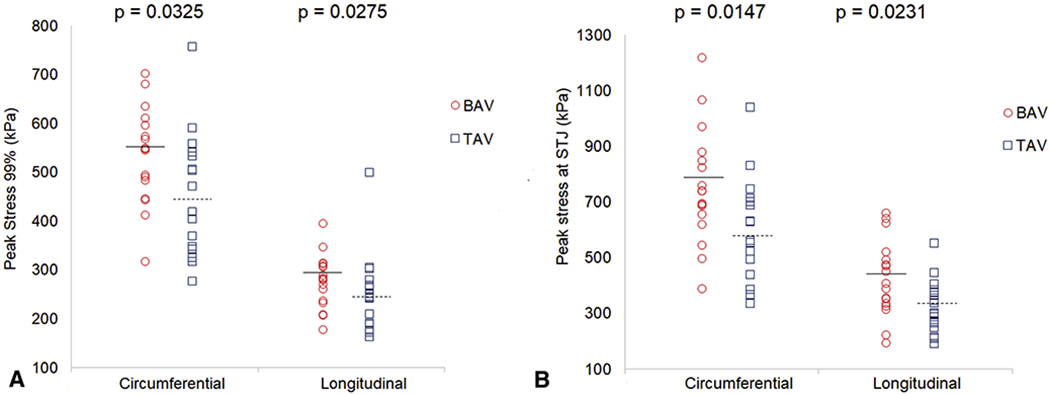
Results: Bicuspid aortic valve-ascending thoracic aortic aneurysms 99th-percentile longitudinal stresses were 280 kPa versus 242 kPa (P = .028) for tricuspid aortic valve-ascending thoracic aortic aneurysms in systole. These stresses did not correlate to diameter for bicuspid aortic valve-ascending thoracic aortic aneurysms (r = -0.004) but had better correlation to tricuspid aortic valve-ascending thoracic aortic aneurysms diameter (r = 0.677). Longitudinal stresses on sinotubular junction were significantly higher in bicuspid aortic valve-ascending thoracic aortic aneurysms than in tricuspid aortic valve-ascending thoracic aortic aneurysms (405 vs 329 kPa, P = .023). Bicuspid aortic valve-ascending thoracic aortic aneurysm 99th-percentile circumferential stresses were 548 kPa versus 462 kPa (P = .033) for tricuspid aortic valve-ascending thoracic aortic aneurysms, which also did not correlate to bicuspid aortic valve-ascending thoracic aortic aneurysm diameter (r = 0.007).
Conclusions: Circumferential and longitudinal stresses were greater in bicuspid aortic valve- than tricuspid aortic valve-ascending thoracic aortic aneurysms and were more pronounced in the sinotubular junction. Peak wall stress did not correlate with bicuspid aortic valve-ascending thoracic aortic aneurysm diameter, suggesting diameter alone in this population may be a poor predictor of dissection risk. Our results highlight the need for patient-specific aneurysm wall stress analysis for accurate dissection risk prediction.
Keywords: aneurysm; bicuspid aortic valve; wall stress.
Copyright © 2018 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
Comment in
-
Assessing wall stresses in bicuspid aortic valve-associated aortopathy: Forecasting the perfect storm?J Thorac Cardiovasc Surg. 2018 Aug;156(2):471-472. doi: 10.1016/j.jtcvs.2018.03.092. Epub 2018 Mar 31. J Thorac Cardiovasc Surg. 2018. PMID: 29666014 No abstract available.
-
Is wall stress like Wall Street when it comes to speculating on bicuspid versus tricuspid aortic valve aneurysm?J Thorac Cardiovasc Surg. 2018 Aug;156(2):501-502. doi: 10.1016/j.jtcvs.2018.04.004. Epub 2018 Apr 12. J Thorac Cardiovasc Surg. 2018. PMID: 29779639 No abstract available.
References
-
- Davies RR, Kaple RK, Mandapati D, et al. Natural history of ascending aortic aneurysms in the setting of an unreplaced bicuspid aortic valve. Ann Thorac Surg. 2007;83(4):1338–1344. - PubMed
-
- Hiratzka LF, Creager MA, Isselbacher EM, et al. Surgery for Aortic Dilatation in Patients With Bicuspid Aortic Valves: A Statement of Clarification From the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;67(6):724–731. doi: 10.1016/j.jacc.2015.11.006 - DOI - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48(3):e1–e148. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(23):e521–643. doi: 10.1161/CIR.0000000000000031 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
