

Deterministic Evolutionary Trajectories Influence Primary Tumor Growth: TRACERx Renal
- PMID: 29656894
- PMCID: PMC5938372
- DOI: 10.1016/j.cell.2018.03.043
Deterministic Evolutionary Trajectories Influence Primary Tumor Growth: TRACERx Renal
Abstract
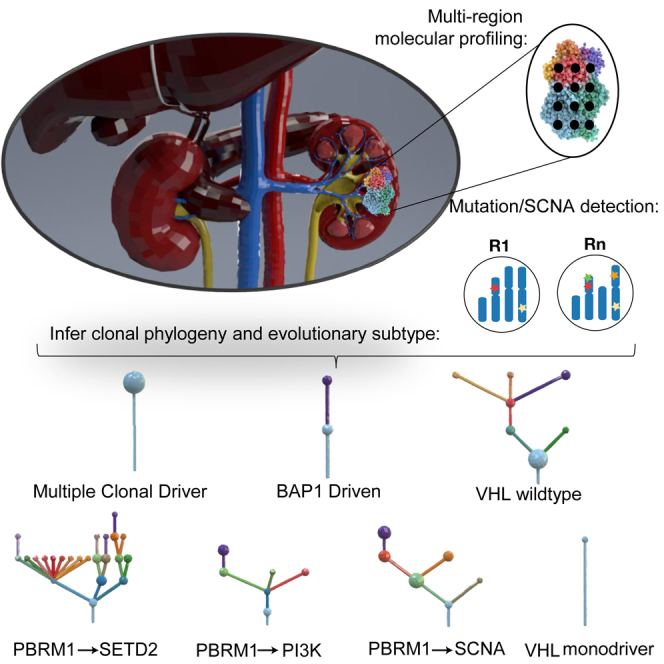
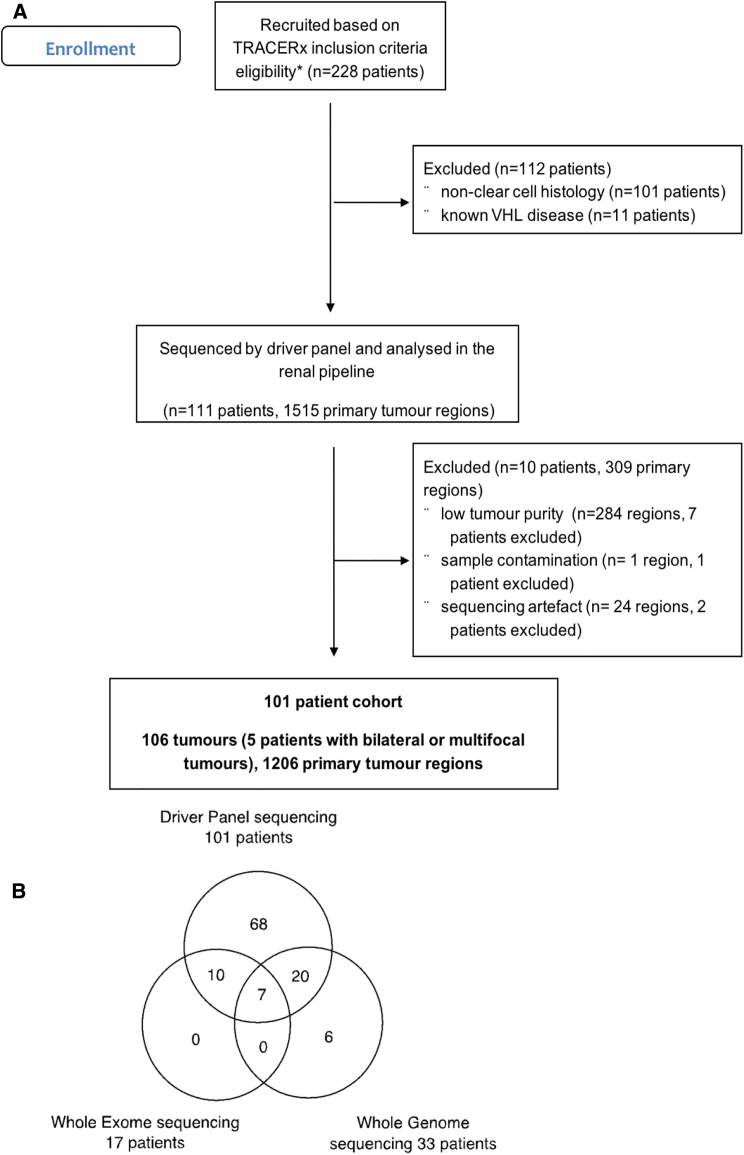
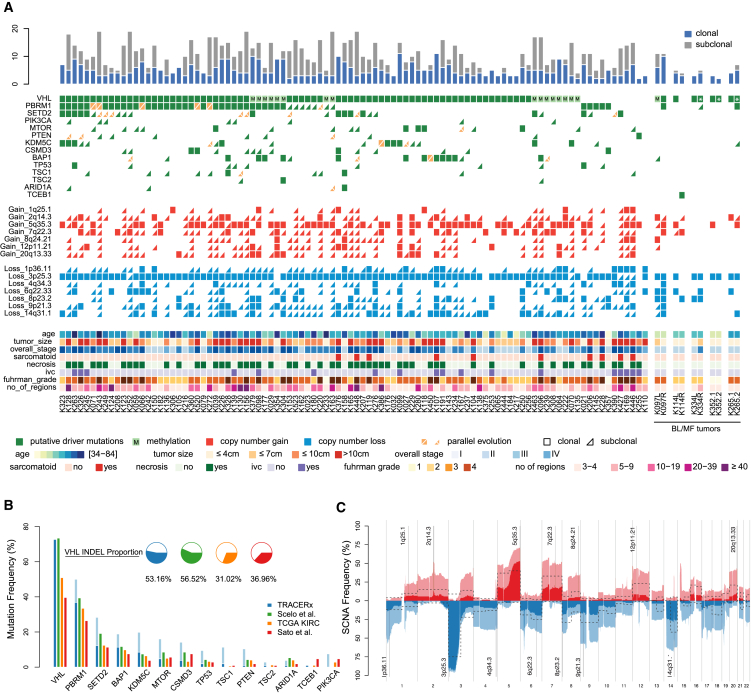
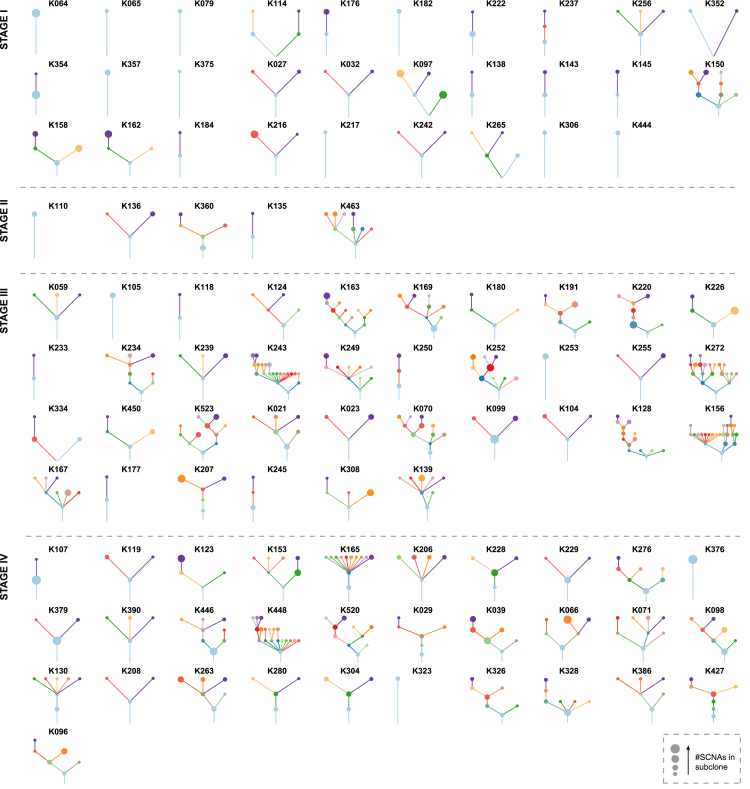
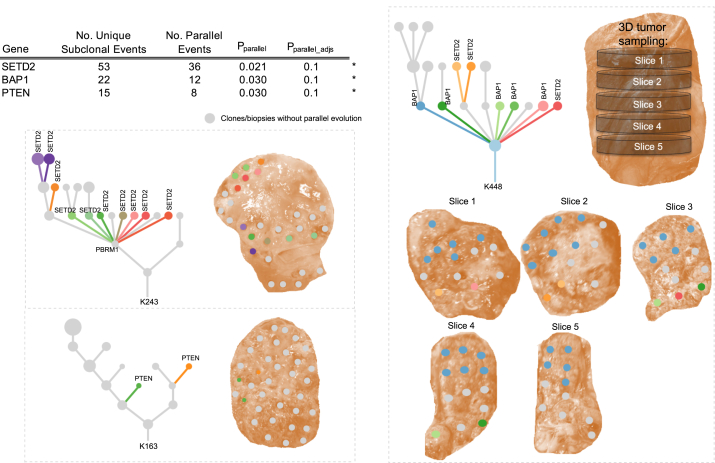
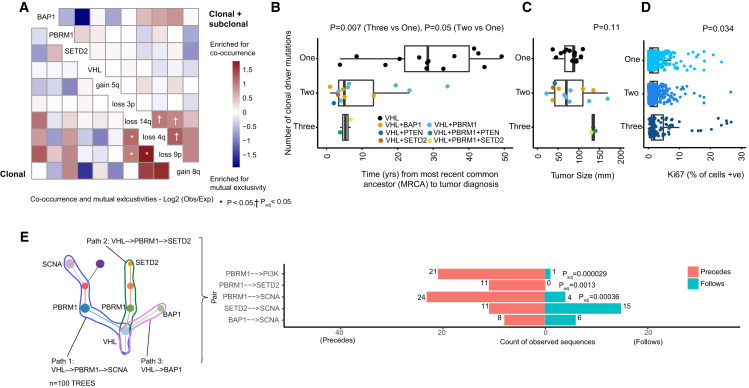
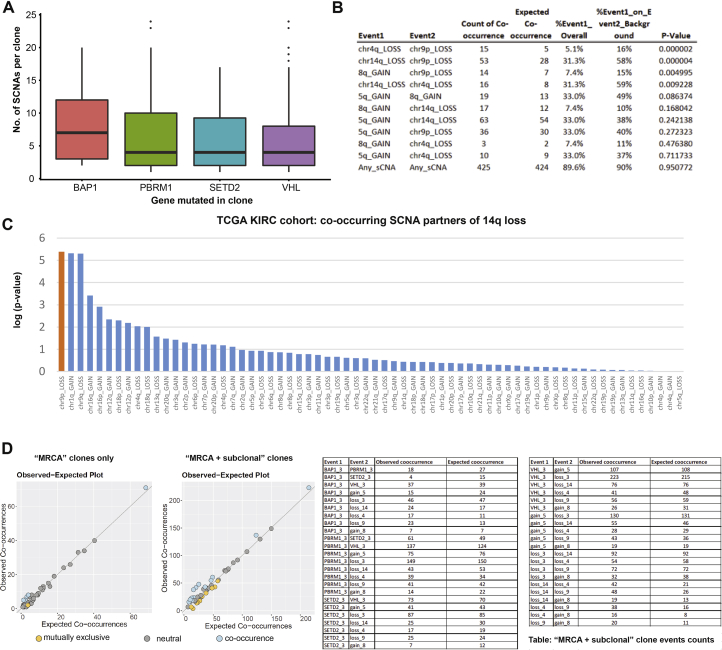
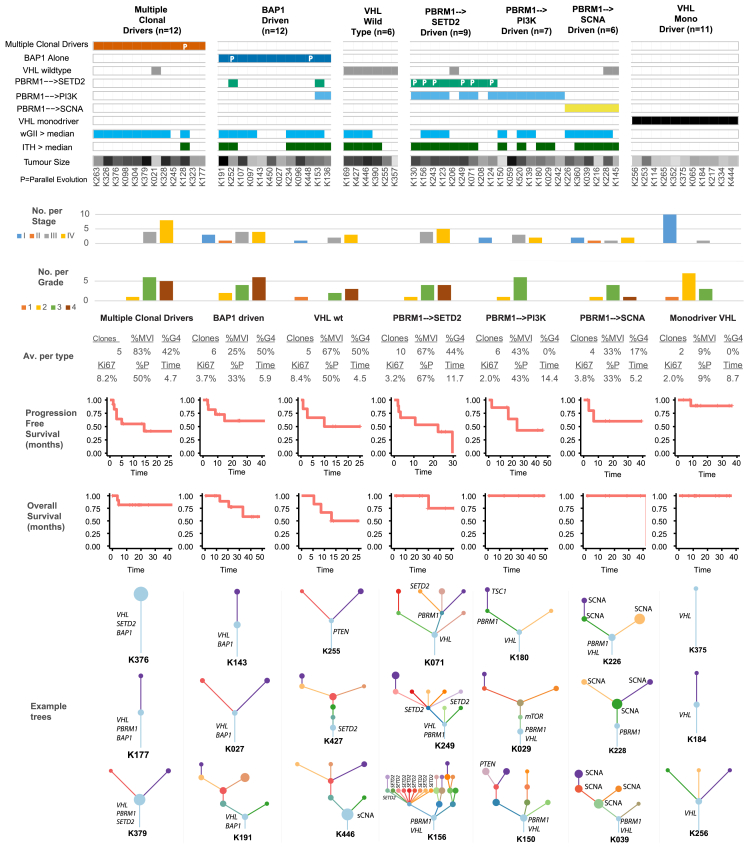
The evolutionary features of clear-cell renal cell carcinoma (ccRCC) have not been systematically studied to date. We analyzed 1,206 primary tumor regions from 101 patients recruited into the multi-center prospective study, TRACERx Renal. We observe up to 30 driver events per tumor and show that subclonal diversification is associated with known prognostic parameters. By resolving the patterns of driver event ordering, co-occurrence, and mutual exclusivity at clone level, we show the deterministic nature of clonal evolution. ccRCC can be grouped into seven evolutionary subtypes, ranging from tumors characterized by early fixation of multiple mutational and copy number drivers and rapid metastases to highly branched tumors with >10 subclonal drivers and extensive parallel evolution associated with attenuated progression. We identify genetic diversity and chromosomal complexity as determinants of patient outcome. Our insights reconcile the variable clinical behavior of ccRCC and suggest evolutionary potential as a biomarker for both intervention and surveillance.
Trial registration: ClinicalTrials.gov NCT03226886.
Keywords: branched evolution; cancer evolution; chromosome instability; deterministic evolution; intratumor heterogeneity; linear evolution; metastasis; punctuated evolution; renal cell cancer; tumor diversity.
Copyright © 2018 Francis Crick Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Multi-regional Sequencing Elucidates the Evolution of Clear Cell Renal Cell Carcinoma.Cell. 2018 Apr 19;173(3):540-542. doi: 10.1016/j.cell.2018.03.077. Cell. 2018. PMID: 29677504
-
Tracing the steps of cancer evolution.Nat Rev Clin Oncol. 2018 Jul;15(7):401. doi: 10.1038/s41571-018-0033-z. Nat Rev Clin Oncol. 2018. PMID: 29700380 No abstract available.
-
Tracing the steps of cancer evolution.Nat Rev Urol. 2018 Jul;15(7):395. doi: 10.1038/s41585-018-0016-y. Nat Rev Urol. 2018. PMID: 29740117 No abstract available.
-
Tracing clear cell renal carcinoma evolution.Nat Med. 2018 Jun;24(6):702. doi: 10.1038/s41591-018-0074-y. Nat Med. 2018. PMID: 29875457 No abstract available.
-
The origin, evolution and route to metastasis of clear cell RCC.Nat Rev Nephrol. 2018 Sep;14(9):538-540. doi: 10.1038/s41581-018-0031-5. Nat Rev Nephrol. 2018. PMID: 29875480 No abstract available.
References
-
- Beroukhim R., Brunet J.P., Di Napoli A., Mertz K.D., Seeley A., Pires M.M., Linhart D., Worrell R.A., Moch H., Rubin M.A. Patterns of gene expression and copy-number alterations in von-hippel lindau disease-associated and sporadic clear cell carcinoma of the kidney. Cancer Res. 2009;69:4674–4681. - PMC - PubMed
-
- Bex A., Ljungberg B., van Poppel H., Powles T., European Association of Urology The role of cytoreductive nephrectomy: European Association of Urology recommendations in 2016. Eur. Urol. 2016;70:901–905. - PubMed
-
- Brastianos P.K., Carter S.L., Santagata S., Cahill D.P., Taylor-Weiner A., Jones R.T., Van Allen E.M., Lawrence M.S., Horowitz P.M., Cibulskis K. Genomic characterization of brain metastases reveals branched evolution and potential therapeutic targets. Cancer Discov. 2015;5:1164–1177. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
