

Tracking Cancer Evolution Reveals Constrained Routes to Metastases: TRACERx Renal
- PMID: 29656895
- PMCID: PMC5938365
- DOI: 10.1016/j.cell.2018.03.057
Tracking Cancer Evolution Reveals Constrained Routes to Metastases: TRACERx Renal
Abstract
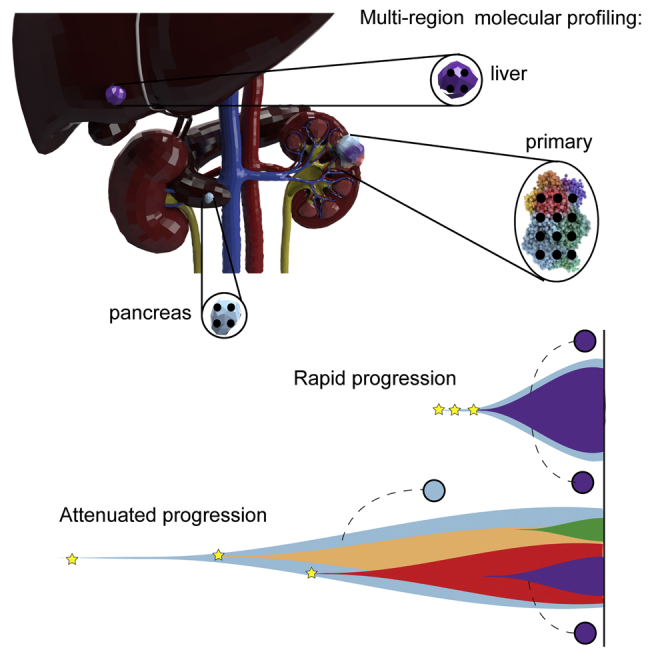
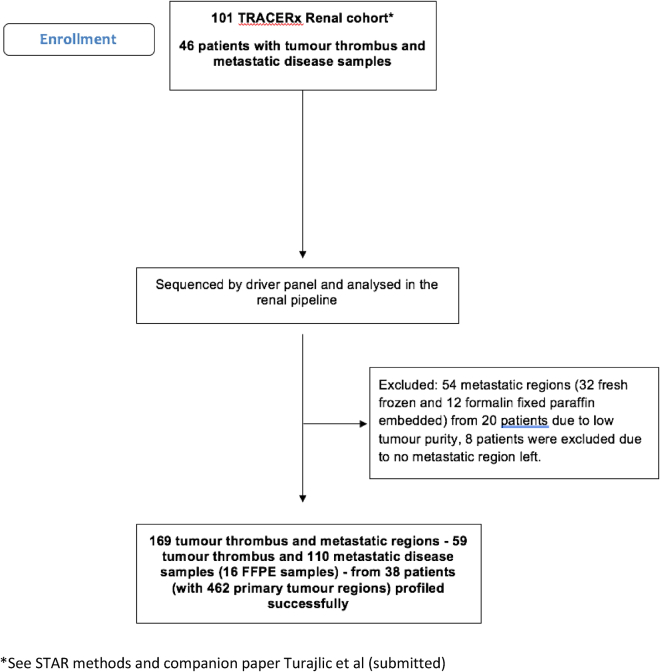
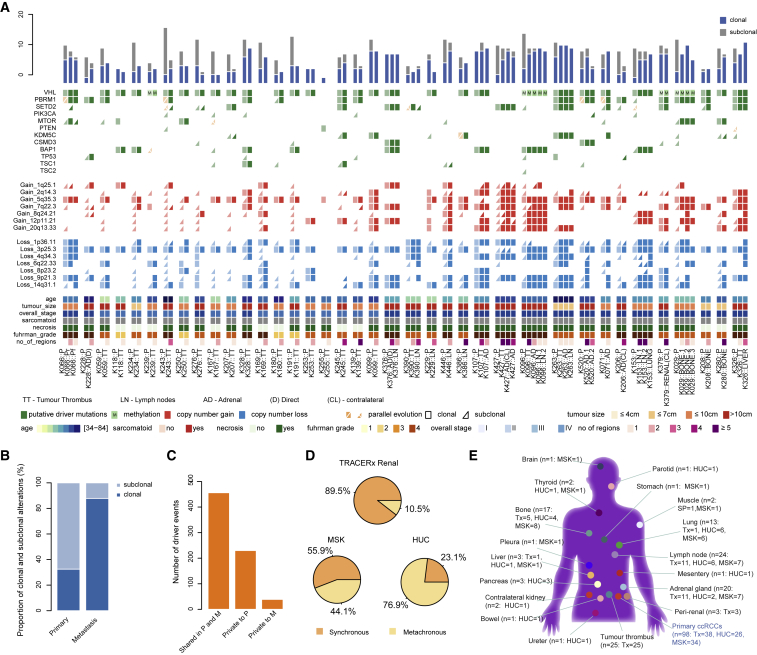
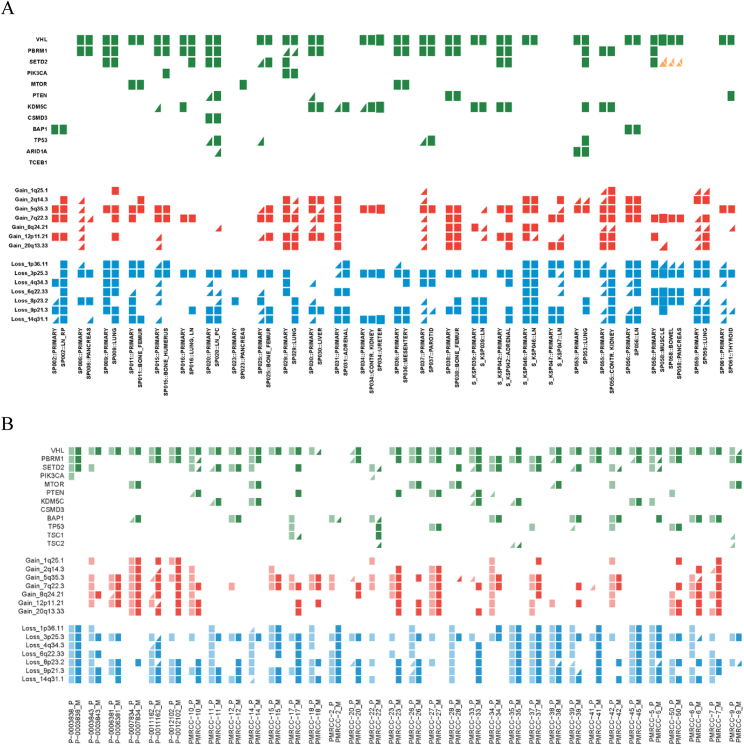
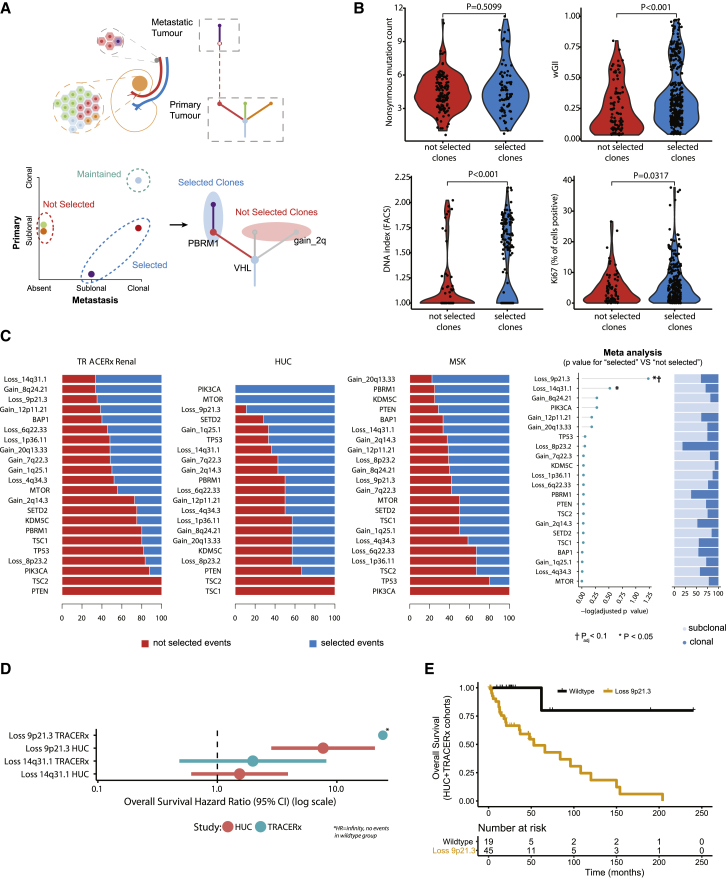
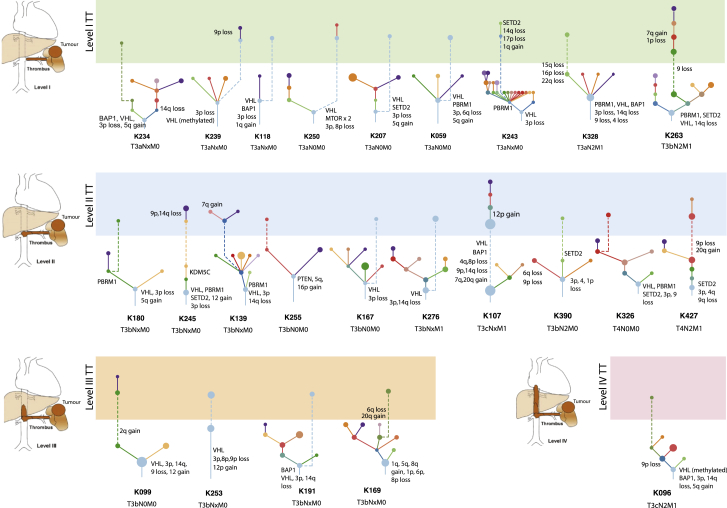
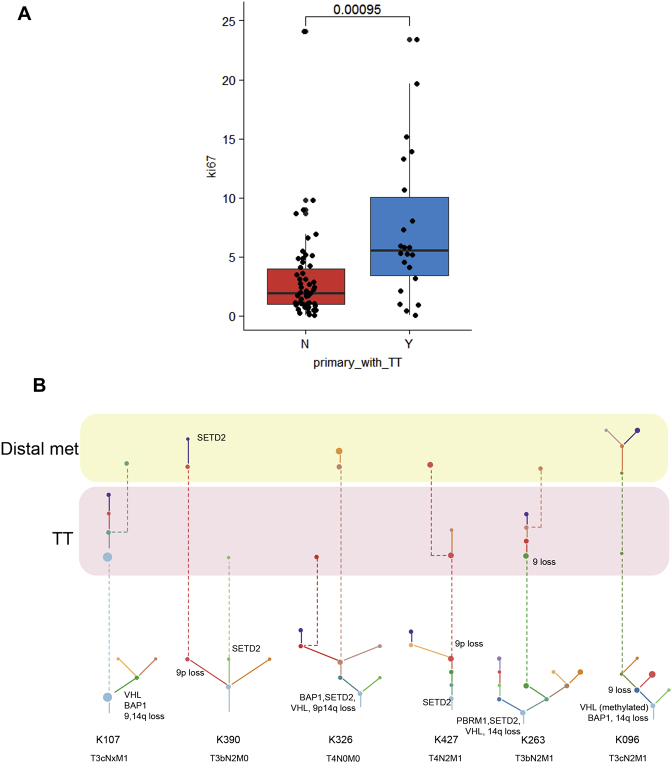
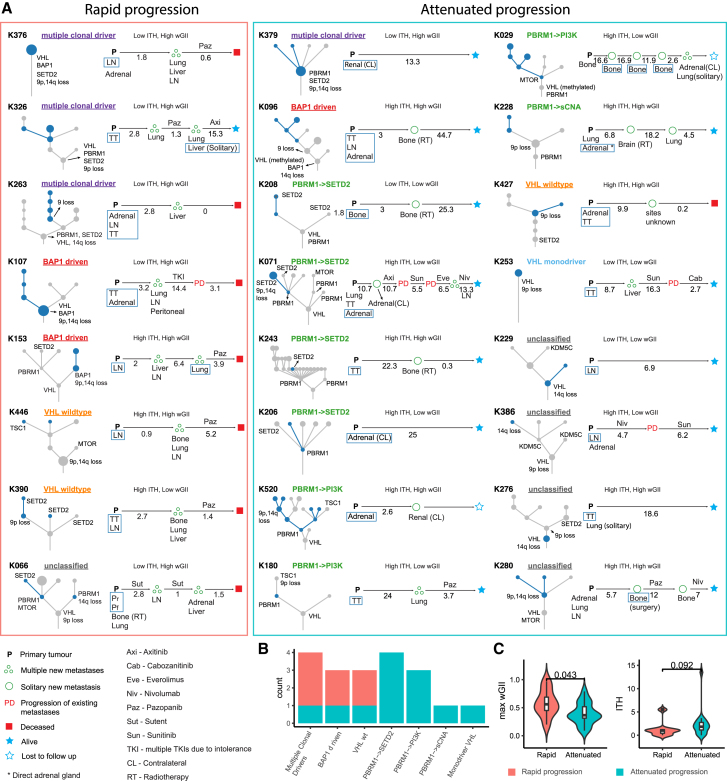
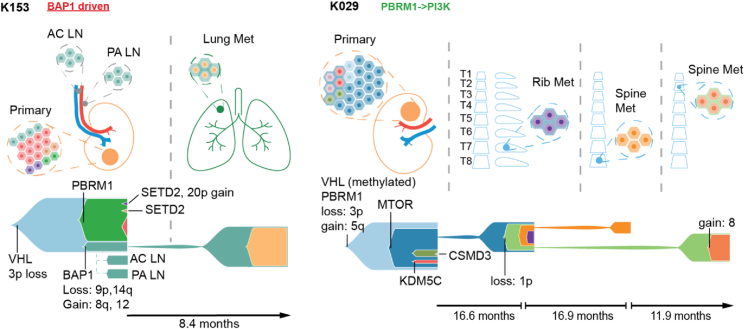
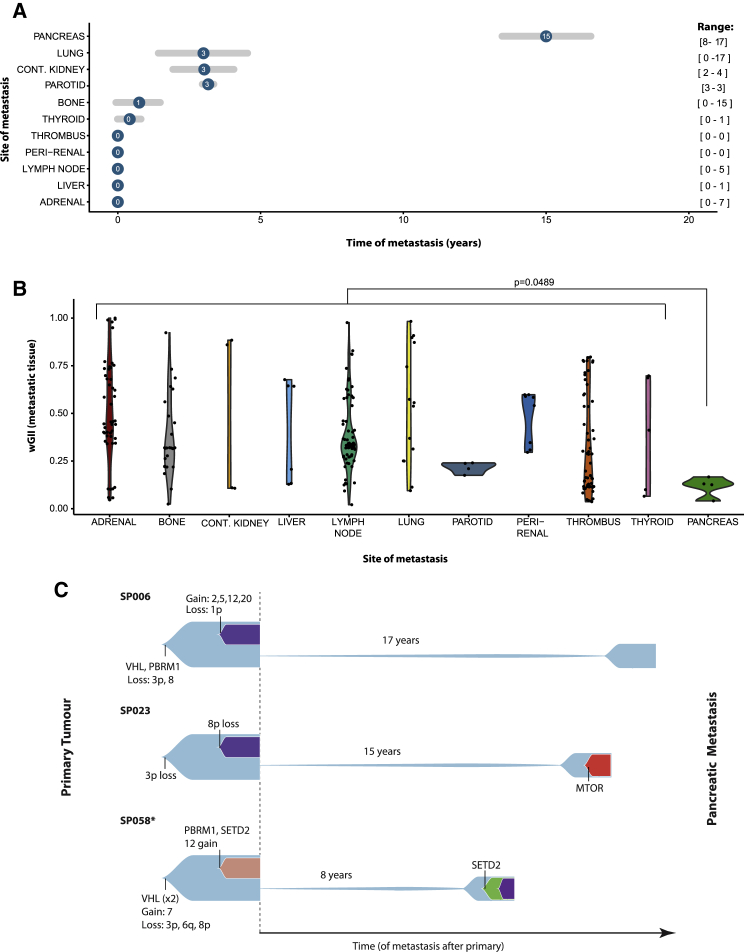
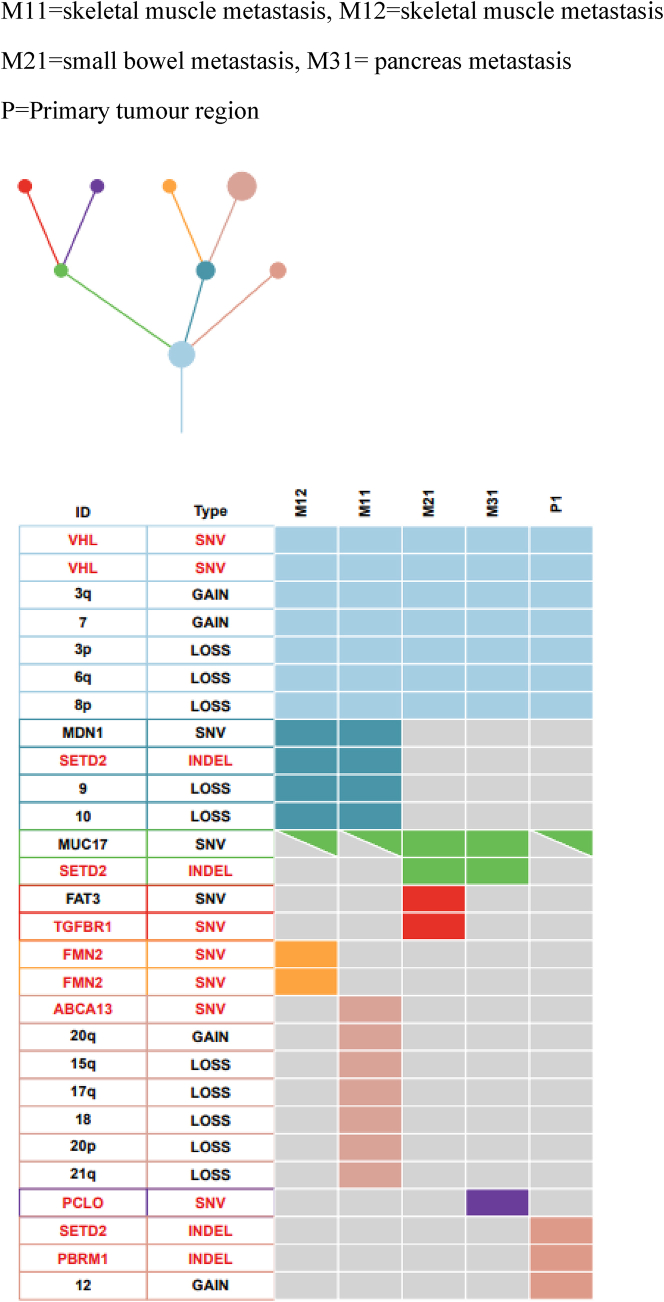
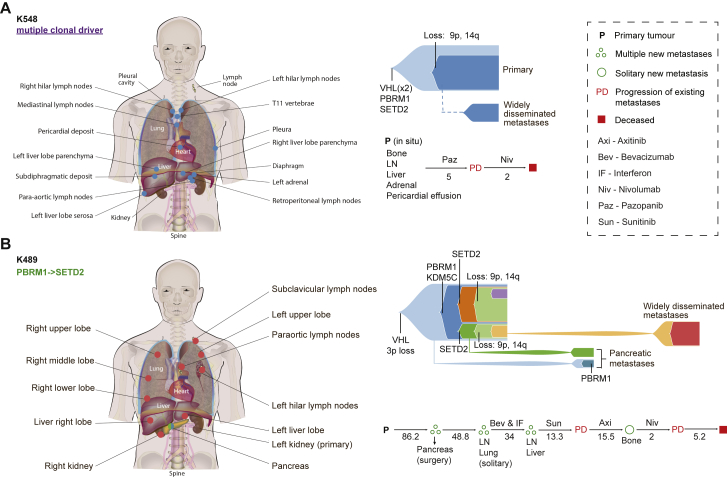
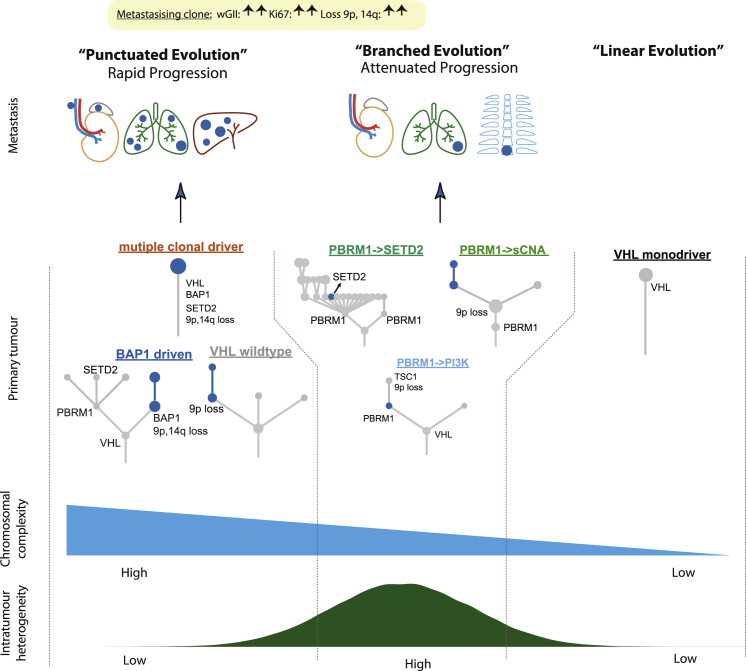
Clear-cell renal cell carcinoma (ccRCC) exhibits a broad range of metastatic phenotypes that have not been systematically studied to date. Here, we analyzed 575 primary and 335 metastatic biopsies across 100 patients with metastatic ccRCC, including two cases sampledat post-mortem. Metastatic competence was afforded by chromosome complexity, and we identify 9p loss as a highly selected event driving metastasis and ccRCC-related mortality (p = 0.0014). Distinct patterns of metastatic dissemination were observed, including rapid progression to multiple tissue sites seeded by primary tumors of monoclonal structure. By contrast, we observed attenuated progression in cases characterized by high primary tumor heterogeneity, with metastatic competence acquired gradually and initial progression to solitary metastasis. Finally, we observed early divergence of primitive ancestral clones and protracted latency of up to two decades as a feature of pancreatic metastases.
Trial registration: ClinicalTrials.gov NCT03226886 NCT03004755.
Keywords: chromosome instability; cytoreductive nephrectomy; evolution of metastasis; loss of 9p; metastasectomy; metastasis; oligometastasis; renal cell cancer; solitary metastasis.
Crown Copyright © 2018. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Multi-regional Sequencing Elucidates the Evolution of Clear Cell Renal Cell Carcinoma.Cell. 2018 Apr 19;173(3):540-542. doi: 10.1016/j.cell.2018.03.077. Cell. 2018. PMID: 29677504
-
Tracing the steps of cancer evolution.Nat Rev Clin Oncol. 2018 Jul;15(7):401. doi: 10.1038/s41571-018-0033-z. Nat Rev Clin Oncol. 2018. PMID: 29700380 No abstract available.
-
Tracing clear cell renal carcinoma evolution.Nat Med. 2018 Jun;24(6):702. doi: 10.1038/s41591-018-0074-y. Nat Med. 2018. PMID: 29875457 No abstract available.
-
The origin, evolution and route to metastasis of clear cell RCC.Nat Rev Nephrol. 2018 Sep;14(9):538-540. doi: 10.1038/s41581-018-0031-5. Nat Rev Nephrol. 2018. PMID: 29875480 No abstract available.
References
-
- Beroukhim R., Brunet J.P., Di Napoli A., Mertz K.D., Seeley A., Pires M.M., Linhart D., Worrell R.A., Moch H., Rubin M.A. Patterns of gene expression and copy-number alterations in von-hippel lindau disease-associated and sporadic clear cell carcinoma of the kidney. Cancer Res. 2009;69:4674–4681. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
