

Improving the prognosis of patients with severely decreased glomerular filtration rate (CKD G4+): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
- PMID: 29656903
- PMCID: PMC5998808
- DOI: 10.1016/j.kint.2018.02.006
Improving the prognosis of patients with severely decreased glomerular filtration rate (CKD G4+): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
Abstract
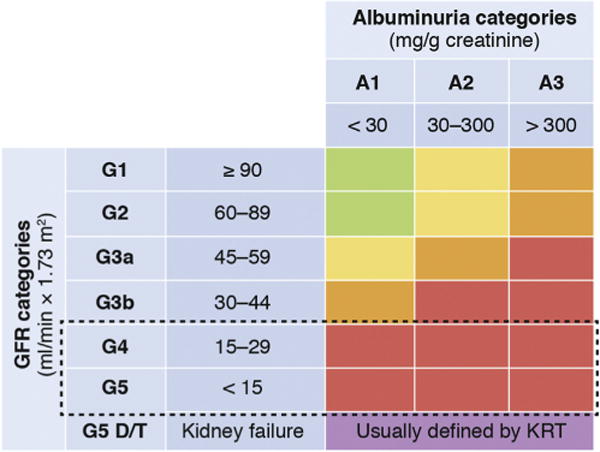
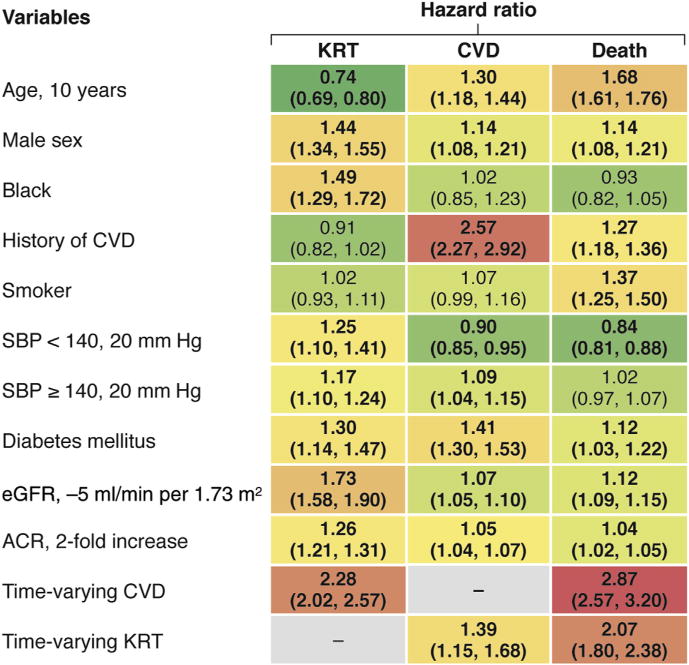
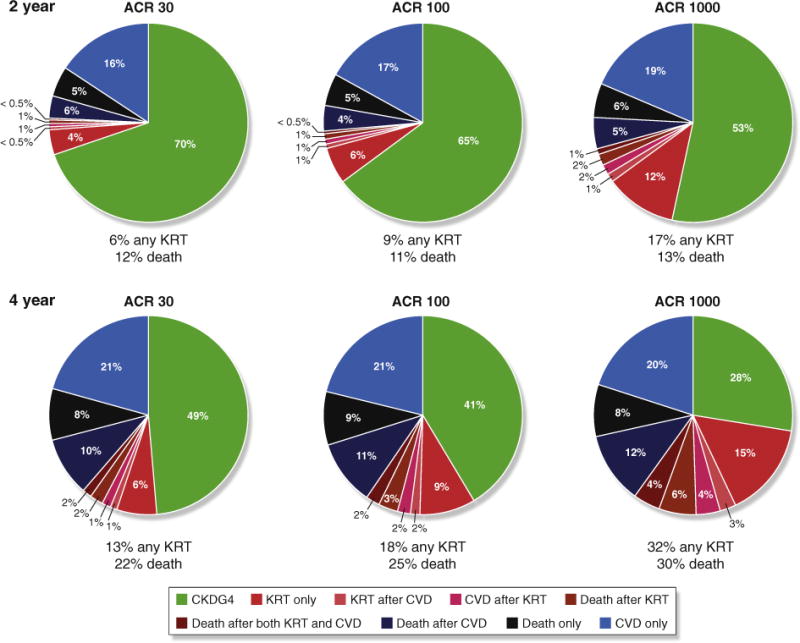
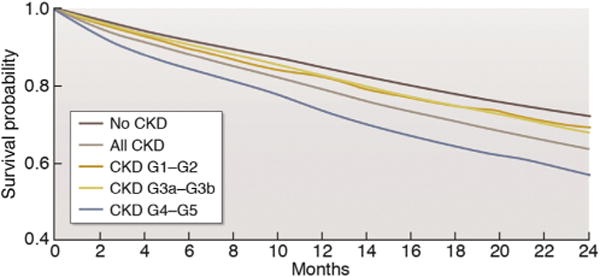
Patients with severely decreased glomerular filtration rate (GFR) (i.e., chronic kidney disease [CKD] G4+) are at increased risk for kidney failure, cardiovascular disease (CVD) events (including heart failure), and death. However, little is known about the variability of outcomes and optimal therapeutic strategies, including initiation of kidney replacement therapy (KRT). Kidney Disease: Improving Global Outcomes (KDIGO) organized a Controversies Conference with an international expert group in December 2016 to address this gap in knowledge. In collaboration with the CKD Prognosis Consortium (CKD-PC) a global meta-analysis of cohort studies (n = 264,515 individuals with CKD G4+) was conducted to better understand the timing of clinical outcomes in patients with CKD G4+ and risk factors for different outcomes. The results confirmed the prognostic value of traditional CVD risk factors in individuals with severely decreased GFR, although the risk estimates vary for kidney and CVD outcomes. A 2- and 4-year model of the probability and timing of kidney failure requiring KRT was also developed. The implications of these findings for patient management were discussed in the context of published evidence under 4 key themes: management of CKD G4+, diagnostic and therapeutic challenges of heart failure, shared decision-making, and optimization of clinical trials in CKD G4+ patients. Participants concluded that variable prognosis of patients with advanced CKD mandates individualized, risk-based management, factoring in competing risks and patient preferences.
Keywords: chronic kidney disease; kidney failure; prediction; prognosis; progression; supportive care.
Copyright © 2018 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
All the other authors declared no competing interests.
Figures
Comment in
-
The estimated glomerular filtration rate graph: another tool in the management of patients with advanced chronic kidney disease.Kidney Int. 2018 Jul;94(1):222. doi: 10.1016/j.kint.2018.04.016. Kidney Int. 2018. PMID: 29933851 No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:1–150.
-
- Levey AS, de Jong PE, Coresh J, et al. The definition, classification, and prognosis of chronic kidney disease: a KDIGO Controversies Conference report. Kidney Int. 2011;80:17–28. - PubMed
-
- Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385:1975–1982. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
