

Significant tumor shift in patients treated with stereotactic radiosurgery for brain metastasis
- PMID: 29657996
- PMCID: PMC5893526
- DOI: 10.1016/j.ctro.2016.12.007
Significant tumor shift in patients treated with stereotactic radiosurgery for brain metastasis
Abstract
Introduction: Linac-based stereotactic radiosurgery (SRS) for brain metastases may be influenced by the time interval between treatment preparation and delivery, related to risk of anatomical changes. We studied tumor position shifts and its relations to peritumoral volume edema changes over time, as seen on MRI.
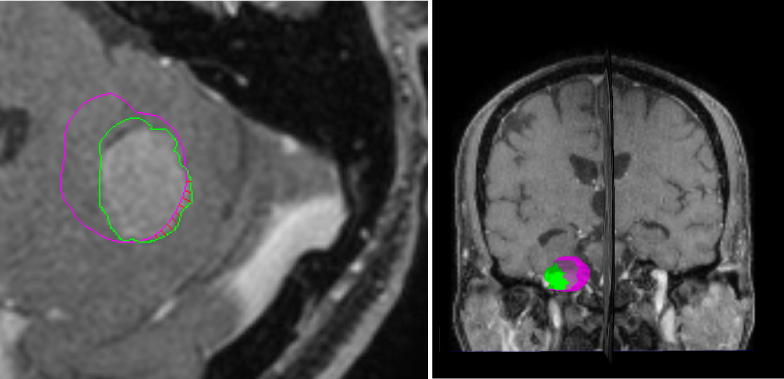
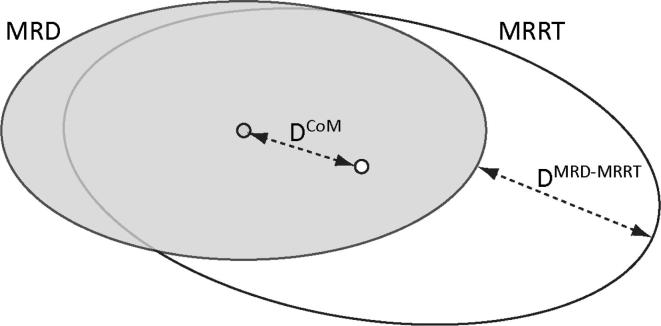
Methods: Twenty-six patients who underwent SRS for brain metastases in our institution were included. We evaluated the occurrence of a tumor shift between the diagnostic MRI and radiotherapy planning MRI. For 42 brain metastases the tumor and peritumoral edema were delineated on the contrast enhanced T1weighted and FLAIR images of both the diagnostic MRI and planning MRI examinations. Centre of Mass (CoM) shifts and tumor borders were evaluated. We evaluated the influence of steroids on peritumoral edema and tumor volume and the correlation with CoM and tumor border changes.
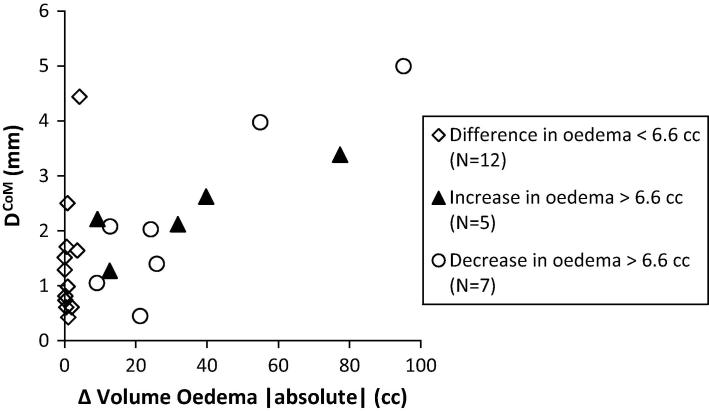
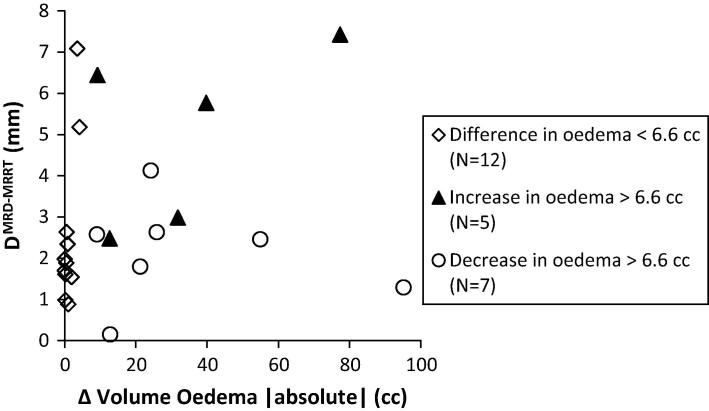
Results: The median values of the CoM shifts and of the maximum distances between the tumor borders obtained from the diagnostic MRI and radiotherapy planning MRI were 1.3 mm (maximum shift of 5.0 mm) and 1.9 mm (maximum distance of 7.4 mm), respectively. We found significant correlations between the absolute change in edema volume and the tumor shift of the CoM (p < 0.001) and tumor border (p = 0.040). Patients who received steroids did not only had a decrease in peritumoral edema, but also had a median decrease in tumor volume of 0.02 cc while patients who did not receive steroids had a median increase of 0.06 cc in tumor volume (p = 0.035).
Conclusion: Our results show that large tumor shifts of brain metastases can occur over time. Because shifts may have a significant impact on the local dose coverage, we recommend minimizing the time between treatment preparation and delivery for Linac based SRS.
Keywords: Brain metastasis; Edema; SRS; Steroids; Tumor shifts.
Figures
References
-
- Oncoline guidelines brain metastases version 3.0 2011. <http://www.oncoline.nl/hersenmetastasen>.
-
- Yamamoto M., Serizawa T., Shuto T. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014;15:387–395. - PubMed
-
- Pinkman M.B., Whitfield G.A., Brada M. New developments in intracranial stereotactic radiotherapy for metastases. Clin Oncol. 2015;27:316–323. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
