

The clinical target volume in lung, head-and-neck, and esophageal cancer: Lessons from pathological measurement and recurrence analysis
- PMID: 29658006
- PMCID: PMC5893525
- DOI: 10.1016/j.ctro.2017.01.006
The clinical target volume in lung, head-and-neck, and esophageal cancer: Lessons from pathological measurement and recurrence analysis
Abstract
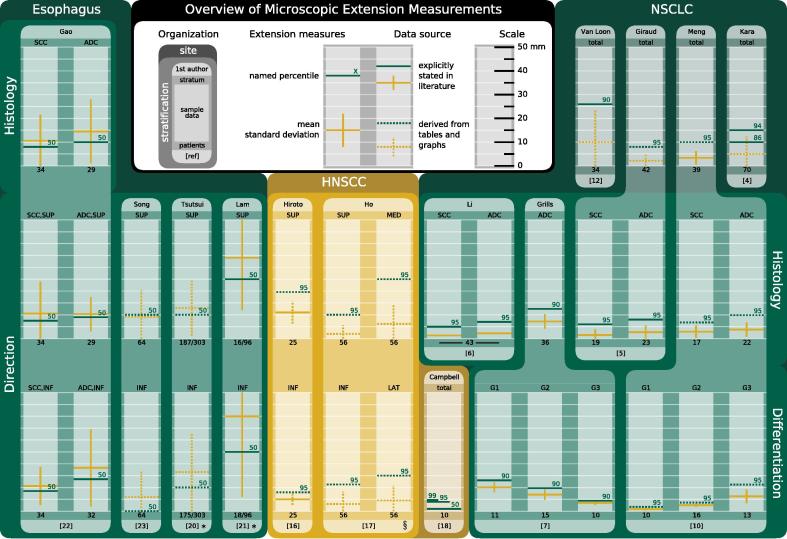
Radiotherapy research has achieved remarkable progress in target volume definition. Advances in medical imaging facilitate more precise localization of the gross tumor volume, alongside a more detailed understanding of the geometric uncertainties associated with treatment delivery that has enabled robust safety margins to be customized to the specific treatment scenario at hand. By contrast, the clinical target volume, meant to encompass gross tumor, as well as, adjacent sub-clinical disease, has evolved very little. It is more often defined by clinician experience and institutional convention than on a patient-specific basis. This disparity arises from the inherent invisibility of sub-clinical disease in current medical imaging. Its incidence and expanse can only be ascertained via indirect means. This article reviews two such strategies: histopathological measurements on resection specimen and analyses of locoregional recurrences after radiotherapy.
Keywords: Adaptive radiotherapy; Clinical target volume; Microscopic tumor extension; Particle beam irradiation.
Figures
References
-
- Troost E., Thorwarth D., Oyen W. Imaging-based treatment adaptation in radiation oncology. J Nucl Med. 2015;56:1922–1929. - PubMed
-
- van Herk M., Remeijer P., Lebesque J. Inclusion of geometric uncertainties in treatment plan evaluation. Int J Radiat Oncol Biol Phys. 2002;52:1407–1422. - PubMed
-
- Moghaddasi F., Bezak E., Marcu L. Current challenges in clinical target volume definition: tumour margins and microscopic extensions. Acta Oncol. 2012;51:984–995. - PubMed
-
- Kara M., Sak S., Orhan D., Yavuzer S. Changing patterns of lung cancer; (3/4 in.) 1.9 cm; still a safe length for bronchial resection margin? Lung Cancer. 2000;30:161–168. - PubMed
-
- Giraud P., Antoine M., Larrouy A., Milleron B., Callard P., De Rycke Y. Evaluation of microscopic tumor extension in non-small-cell lung cancer for three-dimensional conformal radiotherapy planning. Int J Radiat Oncol Biol Phys. 2000;48:1015–1024. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
