

Lumbar sympathectomy versus prostanoids for critical limb ischaemia due to non-reconstructable peripheral arterial disease
- PMID: 29658630
- PMCID: PMC6494604
- DOI: 10.1002/14651858.CD009366.pub2
Lumbar sympathectomy versus prostanoids for critical limb ischaemia due to non-reconstructable peripheral arterial disease
Abstract
Background: Peripheral arterial disease (PAD) is a common circulatory problem that can lead to reduced blood flow to the limbs, which may result in critical limb ischaemia (CLI), a painful manifestation that occurs when a person is at rest. The mainstay of treatment for CLI is surgical or endovascular repair. However, when these means of treatment are not suitable, due to anatomical reasons or comorbidities, treatment for pain is limited. Lumbar sympathectomy and prostanoids have both been shown to reduce pain from CLI in people who suffer from non-reconstructable PAD, but there is currently insufficient evidence to determine if one treatment is superior. Due to the severity of the rest pain caused by CLI, and its impact on quality of life, it is important that people are receiving the best pain relief treatment available, therefore interest in this area of research is high.
Objectives: To compare the efficacy of lumbar sympathectomy with prostanoid infusion in improving symptoms and function and avoiding amputation in people with critical limb ischaemia (CLI) due to non-reconstructable peripheral arterial disease (PAD).
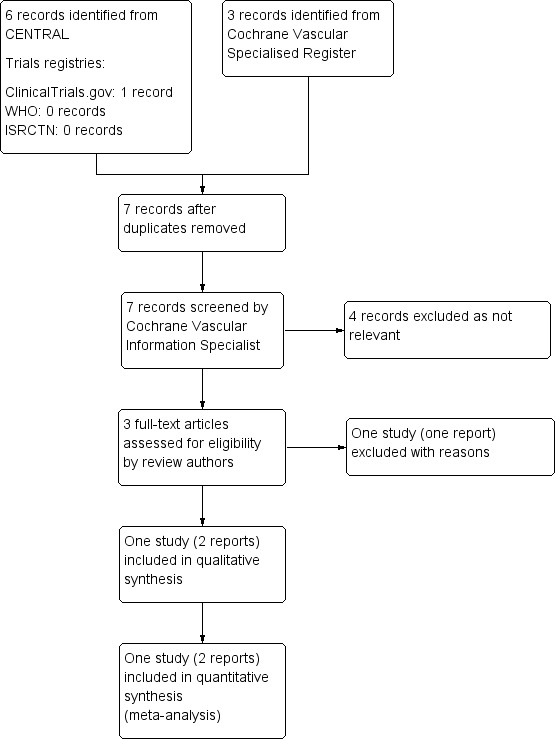
Search methods: The Cochrane Vascular Information Specialist (CIS) searched the Specialised Register (last searched 29 March 2017) and CENTRAL (2017, Issue 2). The CIS also searched clinical trials databases for ongoing or unpublished studies.
Selection criteria: Randomised controlled trials (RCTs), with parallel treatment groups, that compared lumbar sympathectomy (surgical or chemical) with prostanoids (any type and dosage) in people with CLI due to non-reconstructable PAD.
Data collection and analysis: Three review authors independently selected trials, extracted data and assessed risk of bias. Any disagreements were resolved by discussion. We performed fixed-effect model meta-analyses, when there was no overt sign of heterogeneity, with risk ratios (RRs) and 95% confidence intervals (CIs). We graded the quality of evidence according to GRADE.
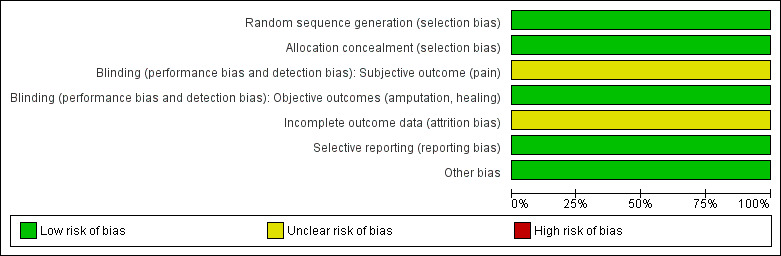
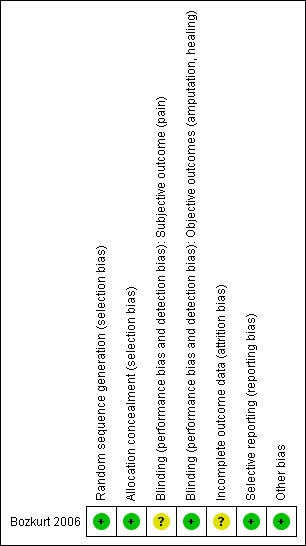
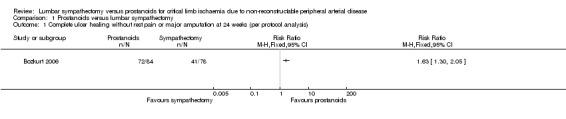
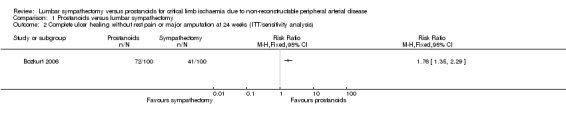
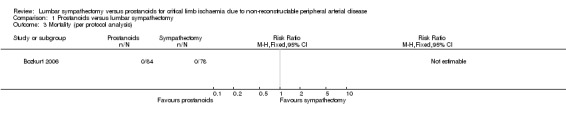
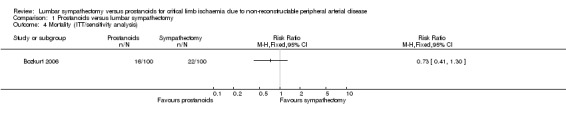
Main results: We included a single study in this review comparing lumbar sympathectomy with prostanoids for the treatment of CLI in people with non-reconstructable PAD. The single study included 200 participants with Buerger's disease, a form of PAD, 100 in each treatment group, but only 162 were actually included in the analyses. The study compared an open surgical technique for lumbar sympathectomy with the prostanoid, iloprost, and followed participants for 24 weeks.Risk of bias was low for most evaluated domains. Due to the nature of the treatment, blinding of the participants and those providing the treatment would be impossible as a surgical procedure was compared with intravenous injections. It was not mentioned if blinded assessors evaluated the study outcomes, therefore, we judged subjective outcomes (i.e. pain reduction) to be at unclear risk of detection bias and objective outcomes (i.e. ulcer healing, amputation and mortality) at low risk of detection bias. We also rated the risk of attrition bias as unclear; 38 out of 200 (19%) participants were not included in the analysis without clear explanation (16 of 100 in the iloprost arm and 22 of 100 in the sympathectomy arm). The quality of evidence was low due to serious imprecision because the study numbers were low and there was only one study included.The single included study reported on the outcome of complete healing without pain or major amputation, which fell under three separate outcomes for our review: relief of rest pain, complete ulcer healing and avoidance of major amputation. We chose to keep the outcome as a singularly reported outcome in order to not introduce bias into the outcomes, which may have been the case if reported separately. The limited evidence suggests participants who received prostaglandins had improved complete ulcer healing without rest pain or major amputation when compared with those who received lumbar sympathectomy (RR 1.63, 95% CI 1.30 to 2.05), but as it was the only included study, we rated the data as low-quality and could not draw any overall conclusions. The study authors stated that more participants who received prostaglandins reported adverse effects, such as headache, flushing, nausea and abdominal discomfort, but only one participant experienced severe enough adverse effects to drop out. Five participants who underwent lumbar sympathectomy reported minor wound infection (low-quality evidence). There was no reported mortality in either of the treatment groups (low-quality evidence).The included study did not report on claudication distances, quality of life or functional status, ankle brachial pressure index (ABPI), tissue oxygenation or toe pressures, or progression to minor amputation, complications or provide any cost-effectiveness data.
Authors' conclusions: Low-quality evidence from a single study in a select group of participants (people with Buerger's disease) suggests that prostaglandins are superior to open surgical lumbar sympathectomy for complete ulcer healing without rest pain or major amputation, but possibly incur more adverse effects. Further studies are needed to better understand if prostaglandins truly are more efficacious than open surgical lumbar sympathectomy and if there are any concerns with adverse effects. It would be of great importance for future studies to include other forms of PAD (as Buerger's disease is a select type of PAD), other methods of sympathectomy as well as data on quality of life, complications and cost-effectiveness.
Conflict of interest statement
IS: none known. SA: none known. PT: PT's institution has received funding from the Indian Council for Medical Research (ICMR): the Professor BV Moses Centre was funded by an educational grant from the Indian Council for Medical Research during the development of the protocol for this Cochrane Review. RF: none known.
Figures
Update of
References
References to studies included in this review
Bozkurt 2006 {published data only}
-
- Bozkurt AK, Koksal C, Demirbas MY, Erdogan A, Rahman A, Demirkilic U, et al. A randomised trial of intravenous Iloprost (a stable prostacyclin analogue) versus lumbar sympathectomy in the management of Buerger's disease. Final Programme and Book of Abstracts. 16th European Chapter Congress of the International Union of Angiology; 2005 Oct 25‐27; Glasgow. 2005. - PubMed
-
- Bozkurt AK, Koksal C, Demirbas MY, Erdogan A, Rahman A, Demirkilic U, et al. A randomized trial of intravenous iloprost (a stable prostacyclin analogue) versus lumbar sympathectomy in the management of Buerger's disease. International Angiology 2006;25(2):162‐8. [PUBMED: 16763533] - PubMed
References to studies excluded from this review
Petronella 2004 {published data only}
-
- Petronella P, Freda F, Nunziata L, Antropoli M, Manganiello A, Cutolo PP, et al. Prostaglandin E1 versus lumbar sympathectomy in the treatment of peripheral arterial occlusive disease: randomised study of 86 patients. Nutrition, Metabolism, and Cardiovascular Diseases: NMCD 2004;14(4):186‐92. [PUBMED: 15553595] - PubMed
Additional references
Abu Dabrh 2015
-
- Abu Dabrh AM, Steffen MW, Asi N, Undavalli C, Wang Z, Elamin MB, et al. Nonrevascularization‐based treatments in patients with severe or critical limb ischemia. Journal of Vascular Surgery 2015;62(5):1330‐9. - PubMed
Aquino 2001
-
- Aquino R, Johnnides C, Makaroun M, Whittle JC, Muluk VS, Kelley ME, et al. Natural history of claudication: long‐term serial follow‐up study of 1244 claudicants. Journal of Vascular Surgery 2001;34(6):962‐70. - PubMed
Deeks 2011
-
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Diehm 2004
-
- Diehm C, Diehm N. Non‐invasive treatment of critical limb ischemia. Current Drug Targets in Cardiovascular and Haematological Disorders 2004;4(3):241‐7. - PubMed
Dormandy 1999
-
- Dormandy J, Heeck L, Vig S. The fate of patients with critical leg ischemia. Seminars in Vascular Surgery 1999;12(2):142‐7. - PubMed
Egger 1997
Faglia 2009
Fontaine 1954
-
- Fontaine VR, Kim M, Kieny R. Surgical treatment for peripheral circulation disorders [Die chirurgische Behandlungder peripheren Durchblutungsstorungen]. Helvetica Chirurgica Acta 1954;21(5‐6):499‐533. - PubMed
Fowkes 2013
-
- Fowkes RG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013;382(9901):1329‐40. - PubMed
GRADEpro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 9 October 2017. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Higgins 2002
-
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Hirsh 2001
-
- Hirsch AT, Criqui MH, Treat‐Jacobson D, Regensteiner JG, Creager MA, Olin JW, et al. Periperal arterial disease detection, awareness, and treatment in primary care. JAMA 2001;286(11):1317‐24. - PubMed
Karanth 2016
Kullo 2016
-
- Kullo IJ, Rooke TW. Peripheral artery disease. New England Journal of Medicine 2016;374(9):861‐71. - PubMed
Lee 2006
-
- Lee AD, Agarwal S, Sadhu D. A 7‐year experience with thoracoscopic sympathectomy for critical upper limb ischemia. World Journal of Surgery 2006;30(9):1644‐7. - PubMed
Liberati 2009
McDermott 2001
-
- McDermott MM, Greenland P, Liu K. Leg symptoms in peripheral arterial disease. JAMA 2001;286(13):1599‐1606. - PubMed
NICE 2012
-
- National Institute for Health and Care Excellence. Peripheral arterial disease: diagnosis and management (CG147). www.nice.org.uk/guidance/cg1479 (accessed 4 August 2017).
Norgren 2007
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter‐society consensus for the management of peripheral arterial disease (TASC II). European Journal of Vascular and Endovascular Surgery 2007;33(Suppl 1):S1‐S75. - PubMed
Pieri 2005
-
- Pieri S, Agresti P, Ialongo P, Fedeli S, Cesare F, Ricci G. Lumbar sympathectomy under CT guidance: therapeutic option in critical limb ischaemia. Radiology in Medicine 2005;109(4):430‐7. - PubMed
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Robertson 2013
Rowe 2009
-
- Rowe V, Lee W, Weaver FA, Etzioni D. Patterns of treatment for peripheral arterial disease in the United States: 1996‐2005. Journal of Vascular Surgery 2009;49(4):910‐7. - PubMed
Ruffolo 2010
Schünemann 2011
-
- Schünemann HJ, Oxman AD, Vist GE, Higgins JP, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Steg 2007
-
- Steg G, Bhatt DL, Wilson WF. One‐year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007;297(11):1197‐206. - PubMed
Tay 2002
-
- Tay VK, Fitridge R, Tie MLH. Computed tomography fluoroscopy‐guided chemical lumbar sympathectomy: simple, safe and effective. Journal of Medical Imaging and Radiation Oncology 2002;46(2):163‐6. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous