When does cognitive decline begin? A systematic review of change point studies on accelerated decline in cognitive and neurological outcomes preceding mild cognitive impairment, dementia, and death
- PMID: 29658744
- PMCID: PMC5906105
- DOI: 10.1037/pag0000236
When does cognitive decline begin? A systematic review of change point studies on accelerated decline in cognitive and neurological outcomes preceding mild cognitive impairment, dementia, and death
Abstract
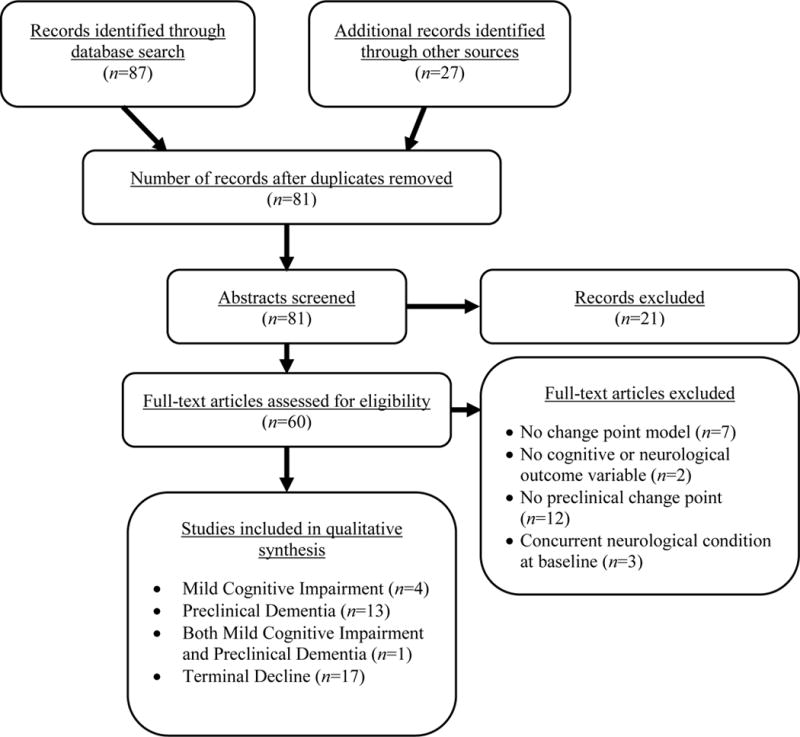
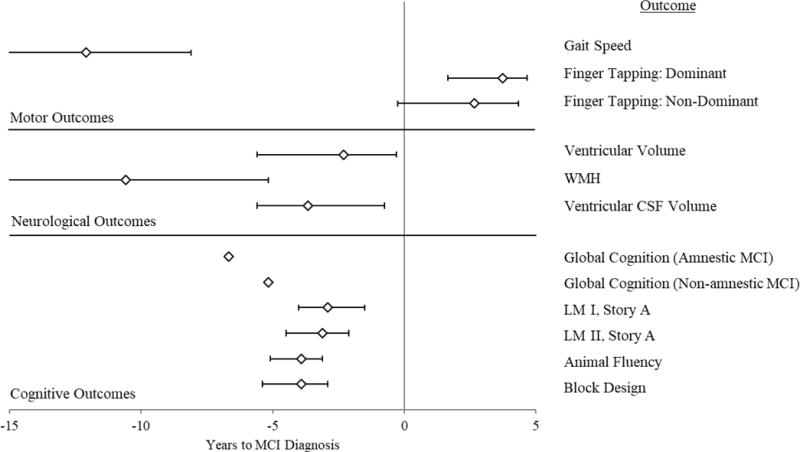
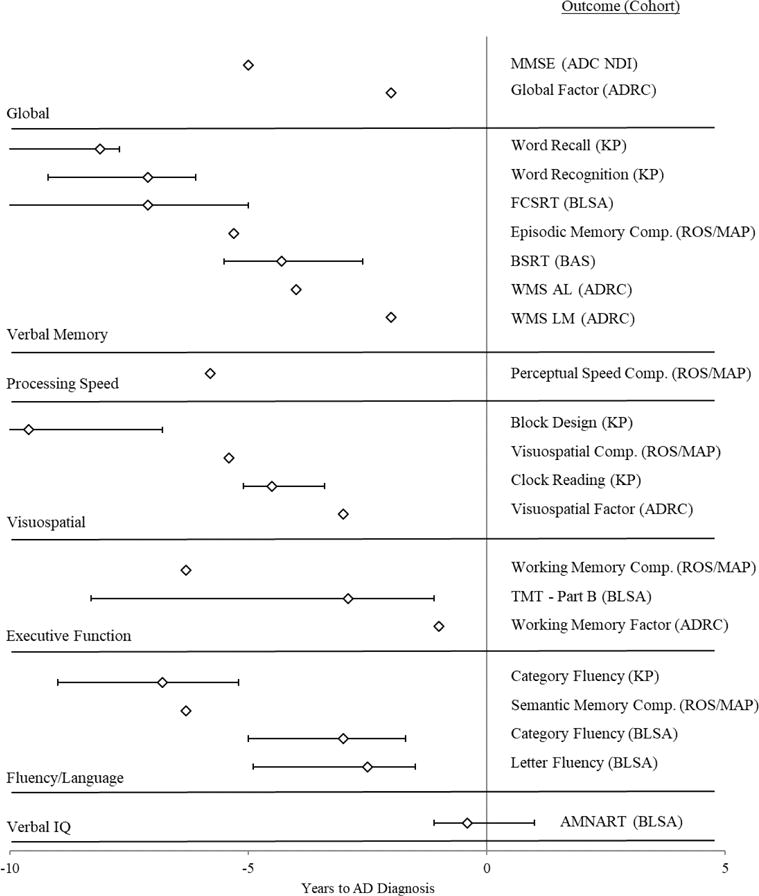
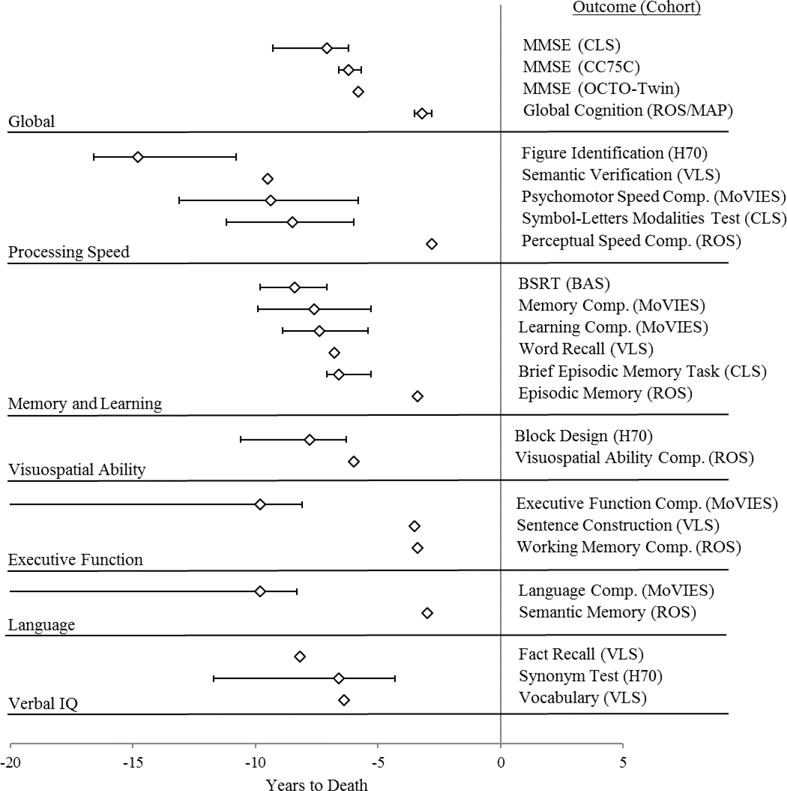
Older adults who ultimately develop dementia experience accelerated cognitive decline long before diagnosis. A similar acceleration in cognitive decline occurs in the years before death as well. To evaluate preclinical and terminal cognitive decline, past researchers have incorporated change points in their analyses of longitudinal data, identifying point estimates of how many years prior to diagnosis or death that decline begins to accelerate. The current systematic review aimed to summarize the published literature on preclinical and terminal change points in relation to mild cognitive impairment (MCI), dementia, and death, identifying the order in which cognitive and neurological outcomes decline and factors that modify the onset and rate of decline. A systematic search protocol yielded 35 studies, describing 16 longitudinal cohorts, modeling change points for cognitive and neurological outcomes preceding MCI, dementia, or death. Change points for cognitive abilities ranged from 3-7 years prior to MCI diagnosis, 1-11 years prior to dementia diagnosis, and 3-15 years before death. No sequence of decline was observed preceding MCI or death, but the following sequence was tentatively accepted for Alzheimer's disease: verbal memory, visuospatial ability, executive functions and fluency, and last, verbal IQ. Some of the modifiers of the onset and rate of decline examined by previous researchers included gender, education, genetics, neuropathology, and personality. Change point analyses evidence accelerated decline preceding MCI, dementia, and death, but moderators of the onset and rate of decline remain ambiguous due to between-study modeling differences, and coordinated analyses may improve comparability across future studies. (PsycINFO Database Record
(c) 2018 APA, all rights reserved).
Figures
References
-
- Aarsland D, Muniz G, Matthews F. Nonlinear decline of mini-mental state examination in Parkinson’s disease. Movement Disorders. 2011;26(2):334–337. http://dx.doi.org/10.1002/mds.23416. - DOI - PubMed
-
- Aguirre-Acevedo DC, Lopera F, Henao E, Tirado V, Muñoz C, Giraldo M, Quiroz YT. Cognitive decline in a Colombian kindred with autosomal dominant Alzheimer disease: A retrospective cohort study. JAMA Neurology. 2016;73(4):431–438. http://dx.doi.org/10.1001/jamaneurol.2015.4851. - DOI - PMC - PubMed
-
- Alzheimer’s Association. 2017 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2017;13(4):325–373. http://dx.doi.org/10.1016/j.jalz.2017.02.001. - DOI
-
- Amariglio RE, Becker JA, Carmasin J, Wadsworth LP, Lorius N, Sullivan C, Johnson KA. Subjective cognitive complaints and amyloid burden in cognitively normal older individuals. Neuropsychologia. 2012;50(12):2880–2886. http://dx.doi.org/10.1016/j.neuropsychologia.2012.08.011. - DOI - PMC - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd. Washington, DC: 1980.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous