

Fully Closed-Loop Multiple Model Probabilistic Predictive Controller Artificial Pancreas Performance in Adolescents and Adults in a Supervised Hotel Setting
- PMID: 29658779
- PMCID: PMC5963546
- DOI: 10.1089/dia.2017.0424
Fully Closed-Loop Multiple Model Probabilistic Predictive Controller Artificial Pancreas Performance in Adolescents and Adults in a Supervised Hotel Setting
Abstract
Background: Initial Food and Drug Administration-approved artificial pancreas (AP) systems will be hybrid closed-loop systems that require prandial meal announcements and will not eliminate the burden of premeal insulin dosing. Multiple model probabilistic predictive control (MMPPC) is a fully closed-loop system that uses probabilistic estimation of meals to allow for automated meal detection. In this study, we describe the safety and performance of the MMPPC system with announced and unannounced meals in a supervised hotel setting.
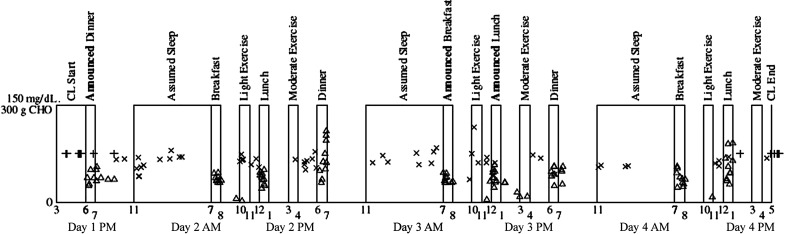
Research design and methods: The Android phone-based AP system with remote monitoring was tested for 72 h in six adults and four adolescents across three clinical sites with daily exercise and meal challenges involving both three announced (manual bolus by patient) and six unannounced (no bolus by patient) meals. Safety criteria were predefined. Controller aggressiveness was adapted daily based on prior hypoglycemic events.
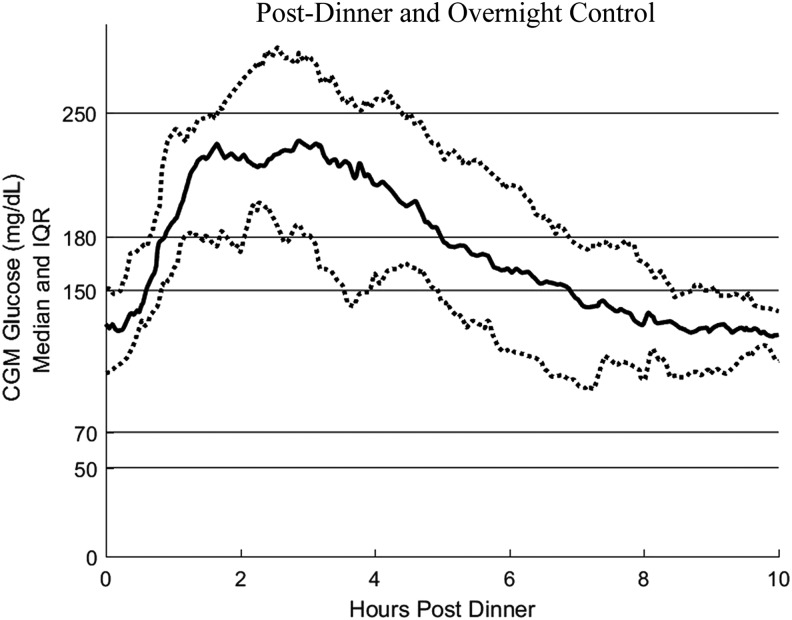
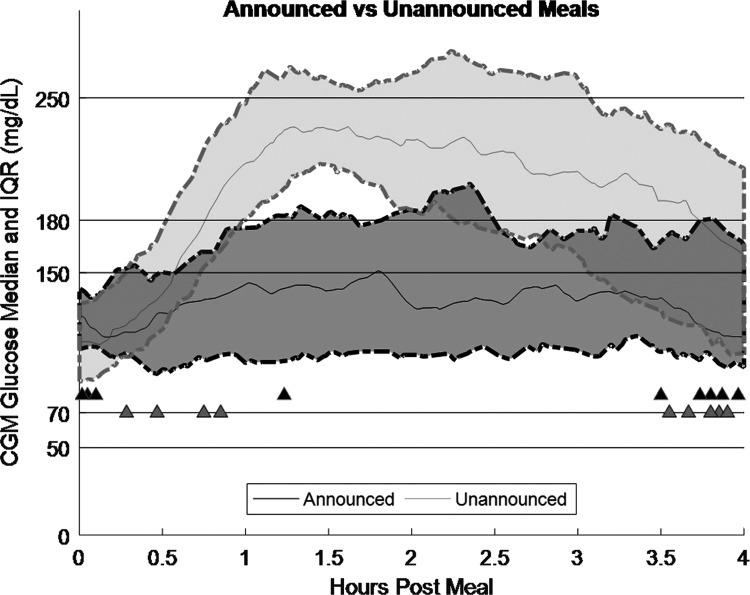
Results: Mean 24-h continuous glucose monitor (CGM) was 157.4 ± 14.4 mg/dL, with 63.6 ± 9.2% of readings between 70 and 180 mg/dL, 2.9 ± 2.3% of readings <70 mg/dL, and 9.0 ± 3.9% of readings >250 mg/dL. Moderate hyperglycemia was relatively common with 24.6 ± 6.2% of readings between 180 and 250 mg/dL, primarily within 3 h after a meal. Overnight mean CGM was 139.6 ± 27.6 mg/dL, with 77.9 ± 16.4% between 70 and 180 mg/dL, 3.0 ± 4.5% <70 mg/dL, 17.1 ± 14.9% between 180 and 250 mg/dL, and 2.0 ± 4.5%> 250 mg/dL. Postprandial hyperglycemia was more common for unannounced meals compared with announced meals (4-h postmeal CGM 197.8 ± 44.1 vs. 140.6 ± 35.0 mg/dL; P < 0.001). No participants met safety stopping criteria.
Conclusions: MMPPC was safe in a supervised setting despite meal and exercise challenges. Further studies are needed in a less supervised environment.
Keywords: Artificial pancreas; Clinical trial; Fully closed-loop; Type 1 diabetes.
Conflict of interest statement
G.P.F. conducts research supported by Medtronic, Tandem, Insulet, and Dexcom and has been a consultant for Abbott and a paid speaker and advisory board member for Dexcom. T.T.L. has received research funding from Medtronic and Tandem, and currently is employed by Insulet. S.D.P. works for Type Zero technologies. C.L. receives research support from Roche, Dexcom, and Senseonics, and is an advisory board member for Novo Nordisk. R.P.W. reports research support from Bigfoot Biomedical, MannKind Corporation, Novo Nordisk, Xeris Pharmaceuticals, and Dexcom and has been a consultant for Eli Lilly and Co and Novo Nordisk. D.M.M. is on the advisory board for Insulet, is a consultant for Abbott Diabetes Care, and receives research funding from Medtronic, Roche, and Dexcom. B.W.B. has served as a consultant for Becton, Dickinson and Company. B.A.B. has received research support from Medtronic, Dexcom, Insulet, Roche, Tandem, and Bigfoot Biomedical and is on advisory boards for Sanofi and Novo Nordisk, and was a consultant for Dexcom. F.M.C., D.L., D.P.H., N.B., G.K., L.M., P.C., and C.L. report no conflicts of interest.
Figures
References
-
- Miller KM, Foster NC, Beck RW, et al. : Current state of type 1 diabetes treatment in the U.S.: updated data from the T1D exchange clinic registry. Diabetes Care 2015;38:971–978 - PubMed
-
- Sherr JL, Hermann JM, Campbell F, et al. : Use of insulin pump therapy in children and adolescents with type 1 diabetes and its impact on metabolic control: comparison of results from three large, transatlantic paediatric registries. Diabetologia 2016;59:87–91 - PubMed
-
- Kowalski AJ: Can we really close the loop and how soon? Accelerating the availability of an artificial pancreas: a roadmap to better diabetes outcomes. Diabetes Technol Ther 2009;11(Suppl 1):S113–S119 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
