

The effectiveness of a group self-management education course for adults with poorly controlled epilepsy, SMILE (UK): A randomized controlled trial
- PMID: 29658989
- PMCID: PMC5969309
- DOI: 10.1111/epi.14073
The effectiveness of a group self-management education course for adults with poorly controlled epilepsy, SMILE (UK): A randomized controlled trial
Abstract
Objective: Epilepsy is one of the most common neurological conditions affecting about 1% of adults. Up to 40% of people with epilepsy (PWE) report recurring seizures while on medication. And optimal functioning requires good self-management. Our objective was to evaluate a group self-management education courses for people with epilepsy and drug-resistant seizures by means of a multicenter, pragmatic, parallel group, randomized controlled trial.
Methods: We recruited adults with epilepsy, having ≥2 seizures in the prior 12 months, from specialist clinics. Consenting participants were randomized 1:1 to a group course or treatment as usual. The primary outcome measure was quality of life 12 months after randomization using Quality of Life 31-P (QOLIE-31-P). Secondary outcome measures were seizure frequency and recency, psychological distress, impact and stigma of epilepsy, self-mastery, medication adherence, and adverse effects. Analysis of outcomes followed the intention-to-treat principle using mixed-effects regression models.
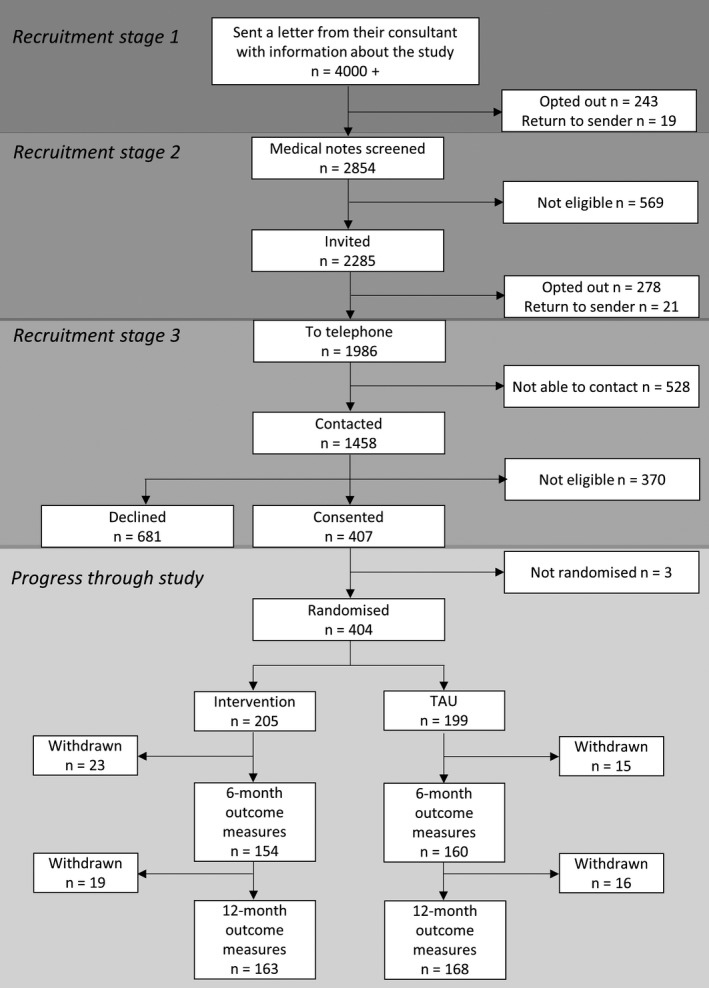
Results: We enrolled 404 participants (intervention: n = 205, control: n = 199) with 331 (82%) completing 12-month follow-up (intervention: n = 163, control: n = 168). Mean age was 41.7 years, ranging from 16 to 85, 54% were female and 75% were white. From the intervention arm, 73.7% attended all or some of the course. At 12-month follow-up, there were no statistically significant differences between trial arms in QOLIE-31-P (intervention mean: 67.4, standard deviation [SD]: 13.5; control mean: 69.5, SD 14.8) or in secondary outcome measures.
Significance: This is the first pragmatic trial of group education for people with poorly controlled epilepsy. Recruitment, course attendance, and follow-up rates were higher than expected. The results show that the primary outcome and quality of life did not differ between the trial arms after 12 months. We found a high prevalence of felt-stigma and psychological distress in this group of people with drug-resistant seizures. To address this, social and psychological interventions require evaluation, and may be necessary before or alongside self-management-education courses.
Keywords: education; epilepsy; quality of life; randomized controlled trial; self-management.
© 2018 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Figures
Comment in
-
Comment on: The effectiveness of a group self-management education course for adults with poorly controlled epilepsy, SMILE (UK): A randomized controlled trial.Epilepsia. 2018 Oct;59(10):1997-1998. doi: 10.1111/epi.14525. Epilepsia. 2018. PMID: 30368789 No abstract available.
References
-
- Moran NF, Poole K, Bell G, et al. Epilepsy in the United Kingdom: seizure frequency and severity, anti‐epileptic drug utilization and impact on life in 1652 people with epilepsy. Seizure. 2004;13:425–33. - PubMed
-
- Thapar A, Kerr M, Harold G. Stress, anxiety, depression, and epilepsy: investigating the relationship between psychological factors and seizures. Epilepsy Behav. 2009;14:134–40. - PubMed
-
- Ettinger AB, Good MB, Manjunath R, et al. The relationship of depression to antiepileptic drug adherence and quality of life in epilepsy. Epilepsy Behav. 2014;36:138–43. - PubMed
-
- Ridsdale L. Avoiding premature death in epilepsy. BMJ. 2015;350:h718. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
