

Continuous electroencephalography predicts delayed cerebral ischemia after subarachnoid hemorrhage: A prospective study of diagnostic accuracy
- PMID: 29659050
- PMCID: PMC6021198
- DOI: 10.1002/ana.25232
Continuous electroencephalography predicts delayed cerebral ischemia after subarachnoid hemorrhage: A prospective study of diagnostic accuracy
Abstract
Objective: Delayed cerebral ischemia (DCI) is a common, disabling complication of subarachnoid hemorrhage (SAH). Preventing DCI is a key focus of neurocritical care, but interventions carry risk and cannot be applied indiscriminately. Although retrospective studies have identified continuous electroencephalographic (cEEG) measures associated with DCI, no study has characterized the accuracy of cEEG with sufficient rigor to justify using it to triage patients to interventions or clinical trials. We therefore prospectively assessed the accuracy of cEEG for predicting DCI, following the Standards for Reporting Diagnostic Accuracy Studies.
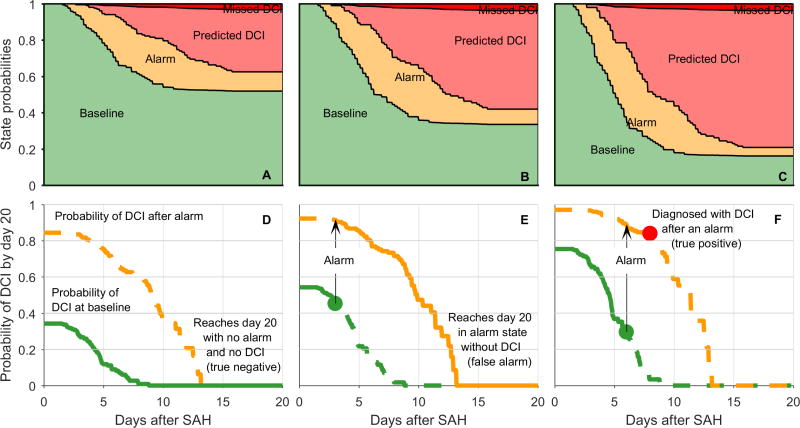
Methods: We prospectively performed cEEG in nontraumatic, high-grade SAH patients at a single institution. The index test consisted of clinical neurophysiologists prospectively reporting prespecified EEG alarms: (1) decreasing relative alpha variability, (2) decreasing alpha-delta ratio, (3) worsening focal slowing, or (4) late appearing epileptiform abnormalities. The diagnostic reference standard was DCI determined by blinded, adjudicated review. Primary outcome measures were sensitivity and specificity of cEEG for subsequent DCI, determined by multistate survival analysis, adjusted for baseline risk.
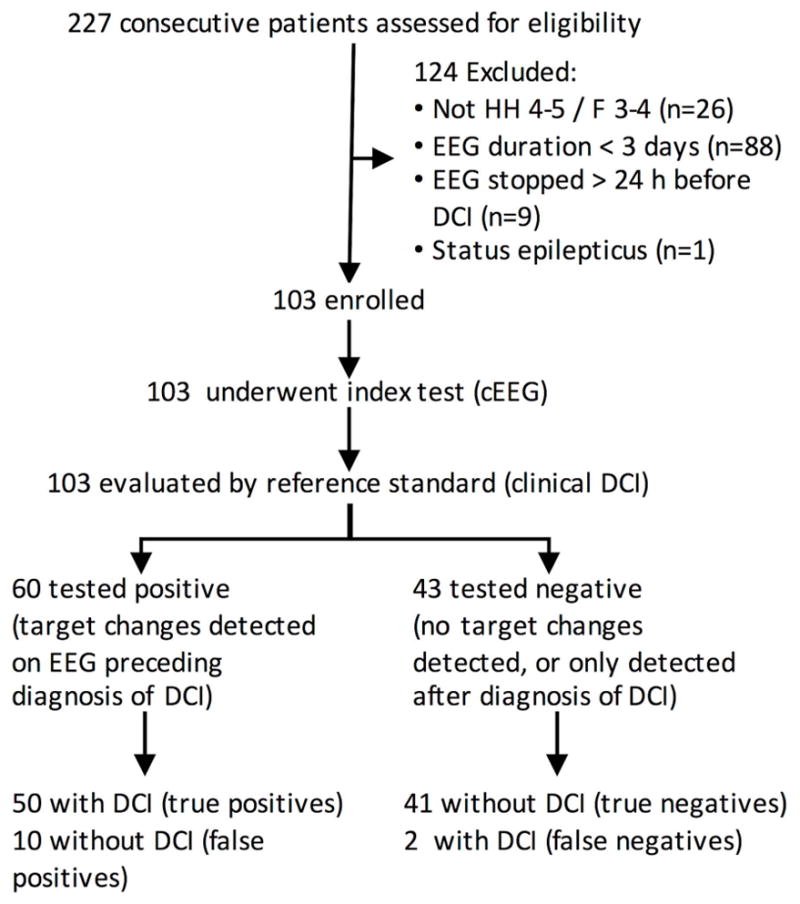
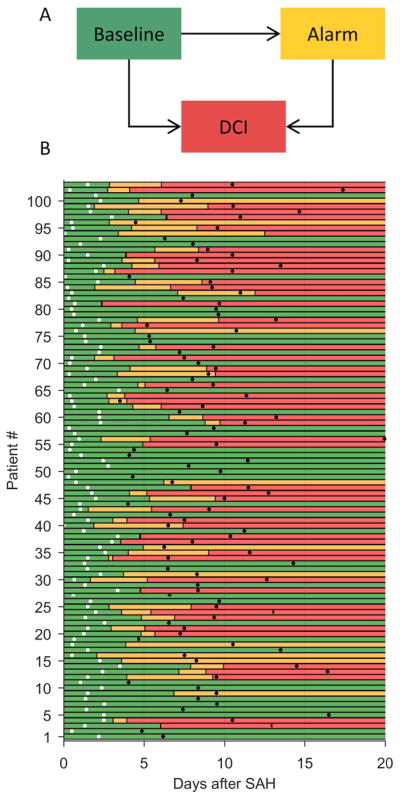
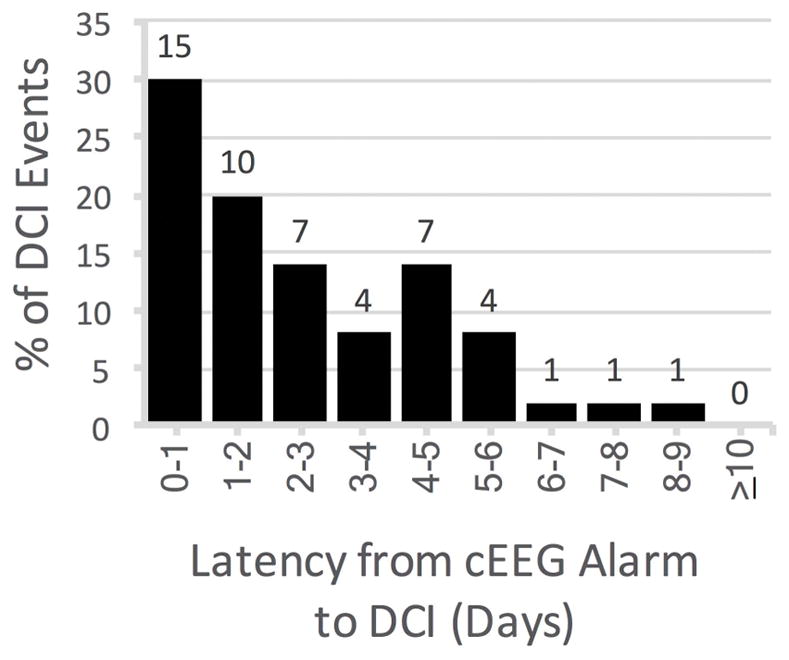
Results: One hundred three of 227 consecutive patients were eligible and underwent cEEG monitoring (7.7-day mean duration). EEG alarms occurred in 96.2% of patients with and 19.6% without subsequent DCI (1.9-day median latency, interquartile range = 0.9-4.1). Among alarm subtypes, late onset epileptiform abnormalities had the highest predictive value. Prespecified EEG findings predicted DCI among patients with low (91% sensitivity, 83% specificity) and high (95% sensitivity, 77% specificity) baseline risk.
Interpretation: cEEG accurately predicts DCI following SAH and may help target therapies to patients at highest risk of secondary brain injury. Ann Neurol 2018;83:958-969.
© 2018 American Neurological Association.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures
References
-
- Feigin VL, Rinkel GJ, Algra A, Vermeulen M, van Gijn J. Calcium antagonists for aneurysmal subarachnoid haemorrhage. The Cochrane Database of Systematic Reviews. 2000;(2):CD000277. - PubMed
-
- Diringer MN, Bleck TP, Claude Hemphill J, 3rd, et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: Recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocritical Care. 2011 Sep;15(2):211–40. - PubMed
-
- Macdonald RL, Higashida RT, Keller E, et al. Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2) Lancet Neurol. 2011 Jul;10(7):618–25. - PubMed
-
- Nuwer MR, Jordan SE, Ahn SS. Evaluation of stroke using EEG frequency analysis and topographic mapping. Neurology. 1987:37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
