

Chronic kidney disease in the global adult HIV-infected population: A systematic review and meta-analysis
- PMID: 29659605
- PMCID: PMC5901989
- DOI: 10.1371/journal.pone.0195443
Chronic kidney disease in the global adult HIV-infected population: A systematic review and meta-analysis
Abstract
Introduction: The widespread use of antiretroviral therapies (ART) has increased life expectancy in HIV patients, predisposing them to chronic non-communicable diseases including Chronic Kidney Disease (CKD). We performed a systematic review and meta-analysis (PROSPERO registration number CRD42016036246) to determine the global and regional prevalence of CKD in HIV patients.
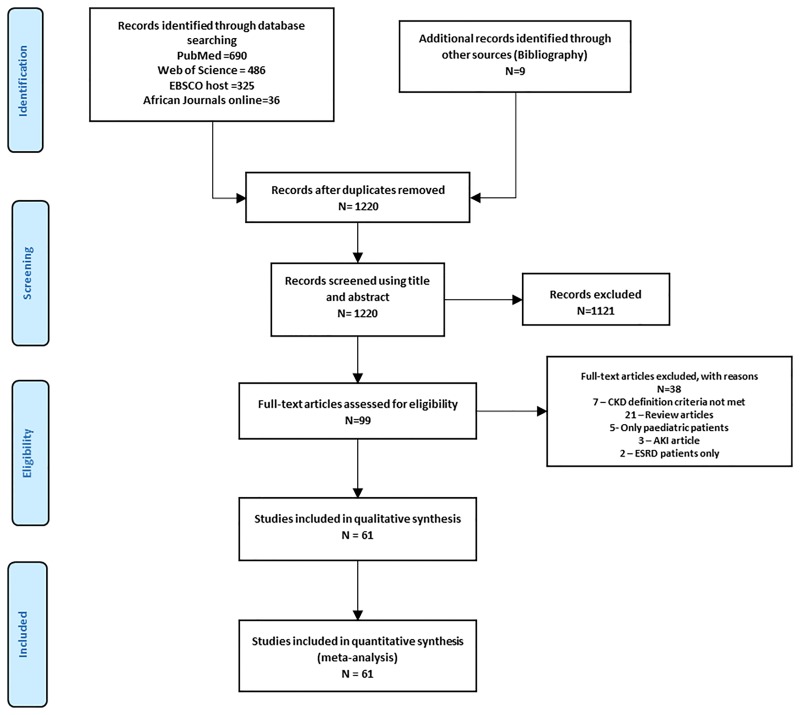
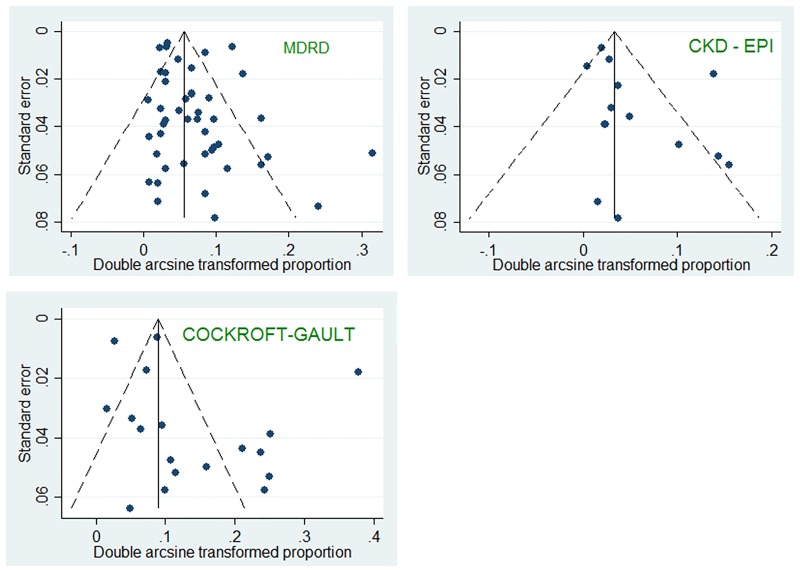
Methods: We searched PubMed, Web of Science, EBSCO and AJOL for articles published between January 1982 and May 2016. CKD was defined as estimated glomerular filtration rate (eGFR) <60ml/min using the MDRD, Cockcroft-Gault or CKD-EPI equations. Random effects model was used to combine prevalence estimates from across studies after variance stabilization via Freeman-Tukey transformation.
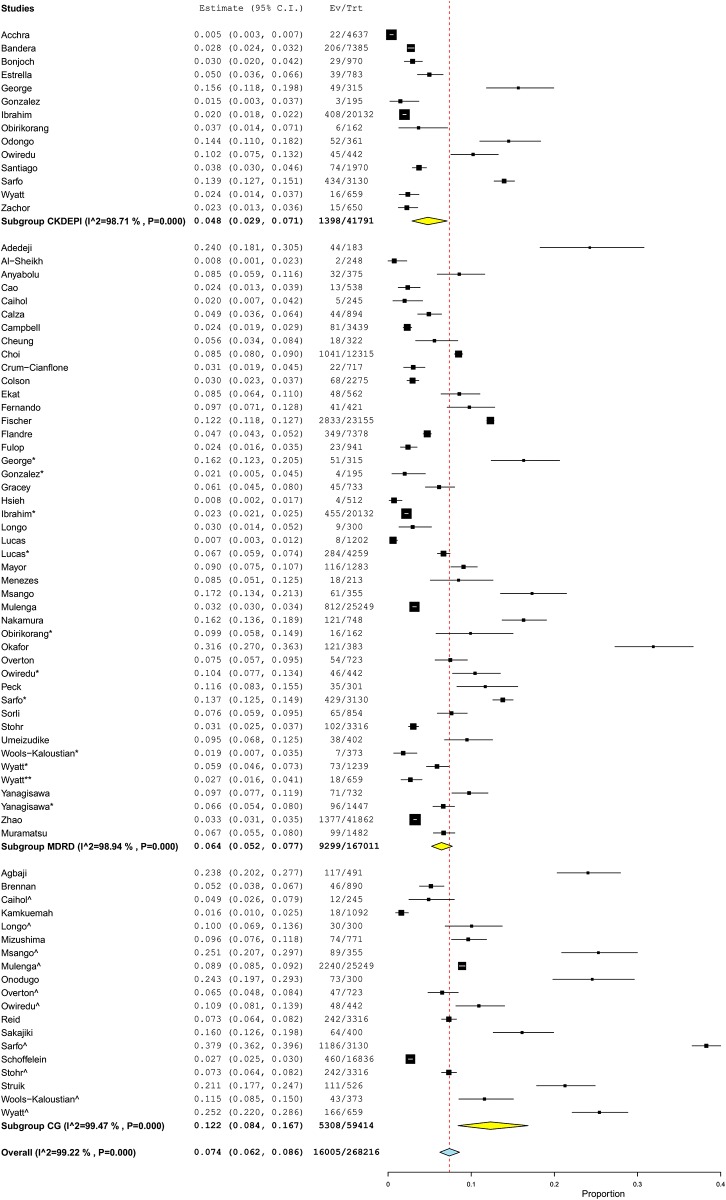
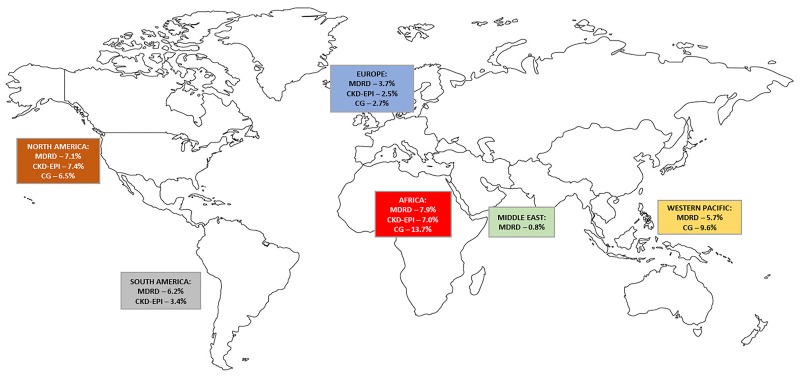
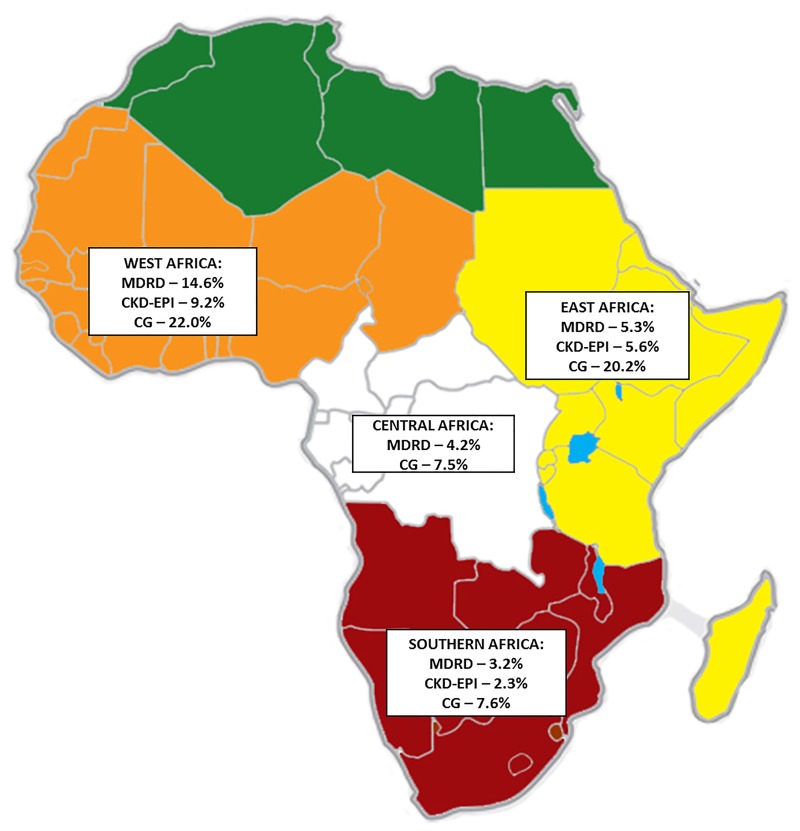
Result: Sixty-one eligible articles (n = 209,078 HIV patients) in 60 countries were selected. The overall CKD prevalence was 6.4% (95%CI 5.2-7.7%) with MDRD, 4.8% (95%CI 2.9-7.1%) with CKD-EPI and 12.3% (95%CI 8.4-16.7%) with Cockcroft-Gault; p = 0.003 for difference across estimators. Sub-group analysis identified differences in prevalence by WHO region with Africa having the highest MDRD-based prevalence at 7.9% (95%CI 5.2-11.1%). Within Africa, the pooled MDRD-based prevalence was highest in West Africa [14.6% (95%CI 9.9-20.0%)] and lowest in Southern Africa (3.2%, 95%CI 3.0-3.4%). The heterogeneity observed could be explained by WHO region, comorbid hypertension and diabetes mellitus, but not by gender, hepatitis B or C coinfection, CD4 count or antiretroviral status.
Conclusion: CKD is common in HIV-infected people, particularly in Africa. HIV treatment programs need to intensify screening for CKD with added need to introduce global guidelines for CKD identification and treatment in HIV positive patients.
Conflict of interest statement
Figures
References
-
- Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. The Lancet. 2015;385(9981):1975–82. - PubMed
-
- Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney international. 2006;69(12):2243–50. doi: 10.1038/sj.ki.5000339 - DOI - PubMed
-
- Szczech LA, Menezes P, Byrd Quinlivan E, van der Horst C, Bartlett JA, Svetkey LP. Microalbuminuria predicts overt proteinuria among patients with HIV infection. HIV medicine. 2010;11(7):419–26. doi: 10.1111/j.1468-1293.2009.00805.x - DOI - PMC - PubMed
-
- Musso CG, Belloso WH, Glassock RJ. Water, electrolytes, and acid-base alterations in human immunodeficiency virus infected patients. World journal of nephrology. 2016;5(1):33–42. doi: 10.5527/wjn.v5.i1.33 - DOI - PMC - PubMed
-
- Li Y, Shlipak MG, Grunfeld C, Choi AI. Incidence and risk factors for acute kidney injury in HIV Infection. American journal of nephrology. 2012;35(4):327–34. doi: 10.1159/000337151 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
