

Infectious Complications After Deployment Trauma: Following Wounded US Military Personnel Into Veterans Affairs Care
- PMID: 29659771
- PMCID: PMC6160604
- DOI: 10.1093/cid/ciy280
Infectious Complications After Deployment Trauma: Following Wounded US Military Personnel Into Veterans Affairs Care
Abstract
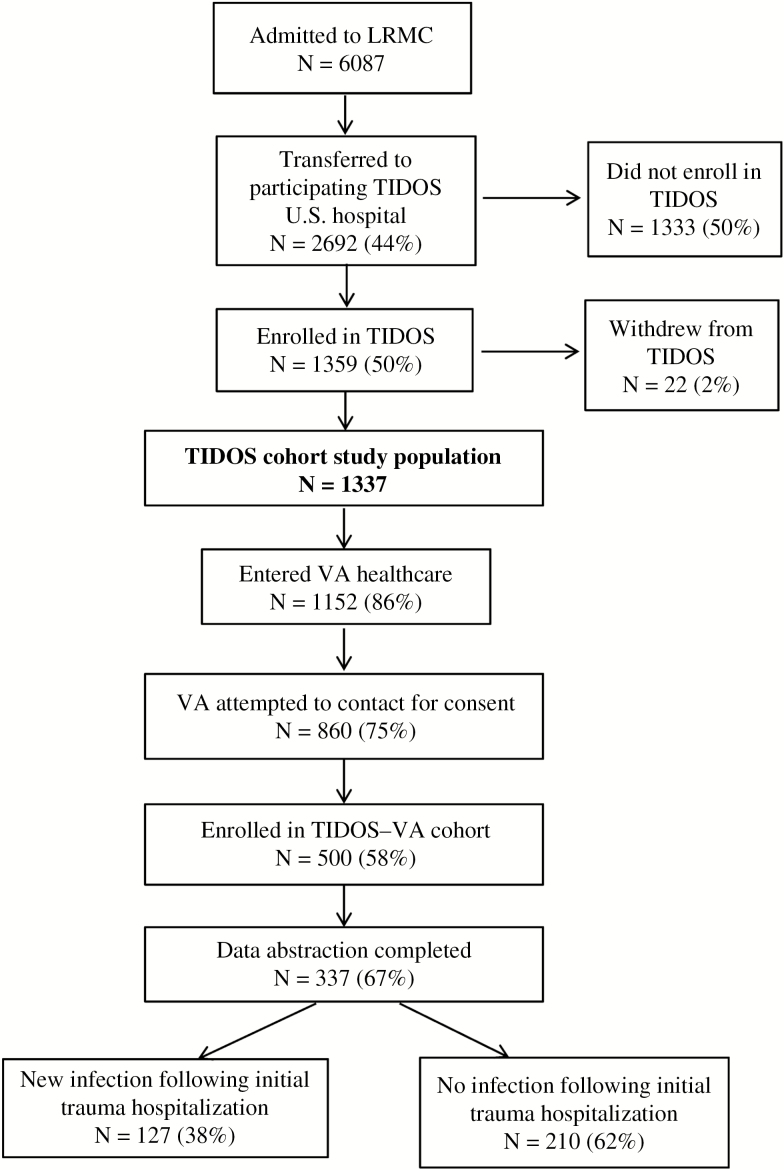
Background: Infectious complications related to deployment trauma significantly contribute to the morbidity and mortality of wounded service members. The Trauma Infectious Disease Outcomes Study (TIDOS) collects data on US military personnel injured in Iraq and Afghanistan in an observational cohort study of infectious complications. Patients enrolled in TIDOS may also consent to follow-up through the Department of Veterans Affairs (VA). We present data from the first 337 TIDOS enrollees to receive VA healthcare.
Methods: Data were collected from the Department of Defense (DoD) Trauma Registry, TIDOS infectious disease module, DoD and VA electronic medical records, and telephone interview. Cox proportional hazard analysis was performed to identify predictors of post-discharge infections related to deployment trauma.
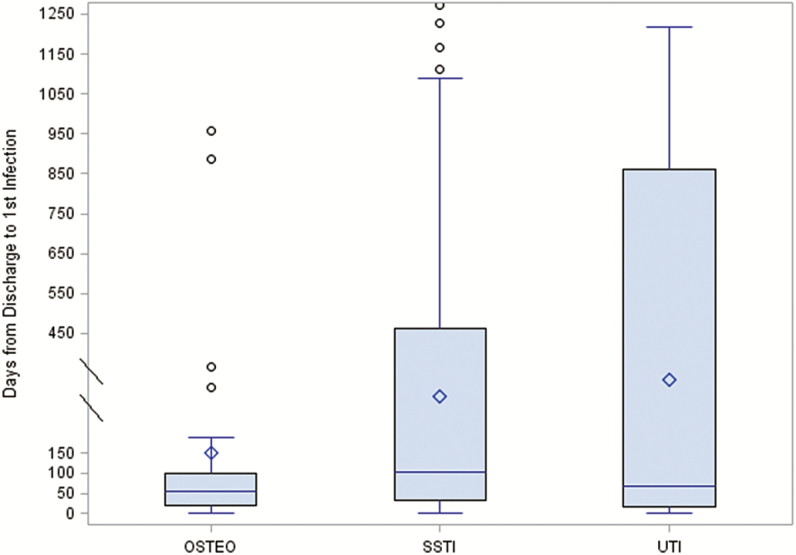
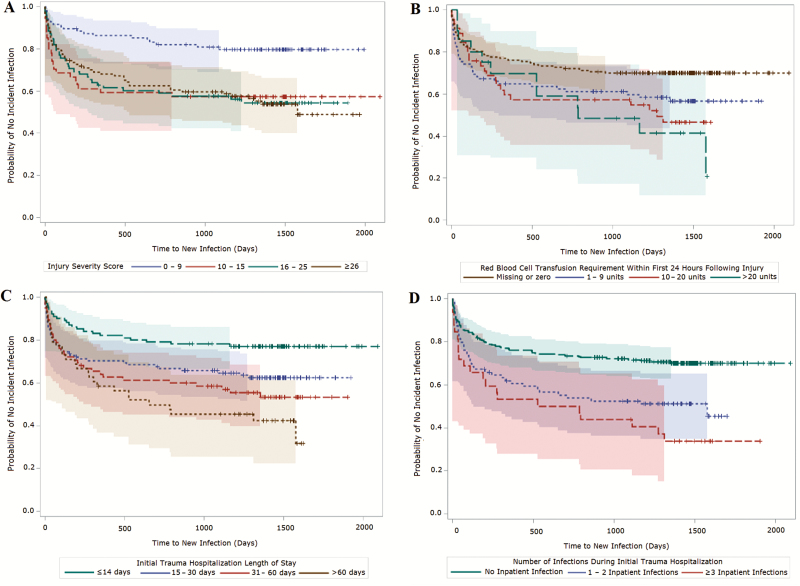
Results: Among the first 337 TIDOS enrollees who entered VA healthcare, 111 (33%) had 244 trauma-related infections during their initial trauma hospitalization (2.1 infections per 100 person-days). Following initial discharge, 127 (38%) enrollees had 239 trauma-related infections (170 during DoD follow-up and 69 during VA time). Skin and soft-tissue infections and osteomyelitis were predominant during and after the initial trauma hospitalization. In a multivariate model, a shorter time to development of a new infection following discharge was independently associated with injury severity score ≥10 and occurrence of ≥1 inpatient infection during initial trauma hospitalization.
Conclusions: Incident infections related to deployment trauma continue well after initial hospital discharge and into VA healthcare. Overall, 38% of enrolled patients developed a new trauma-related infection after their initial hospital discharge, with 29% occurring after the patient left military service.
Figures
References
-
- Murray CK, Hinkle MK, Yun HC. History of infections associated with combat-related injuries. J Trauma 2008; 64:S221–31. - PubMed
-
- Murray CK. Epidemiology of infections associated with combat-related injuries in Iraq and Afghanistan. J Trauma 2008; 64:S232–8. - PubMed
-
- Murray CK, Wilkins K, Molter NC, et al. Infections in combat casualties during Operations Iraqi and Enduring Freedom. J Trauma 2009; 66:S138–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
