

Integration of physical abuse clinical decision support into the electronic health record at a Tertiary Care Children's Hospital
- PMID: 29659856
- PMCID: PMC7647034
- DOI: 10.1093/jamia/ocy025
Integration of physical abuse clinical decision support into the electronic health record at a Tertiary Care Children's Hospital
Abstract
Objective: To evaluate the effect of a previously validated electronic health record-based child abuse trigger system on physician compliance with clinical guidelines for evaluation of physical abuse.
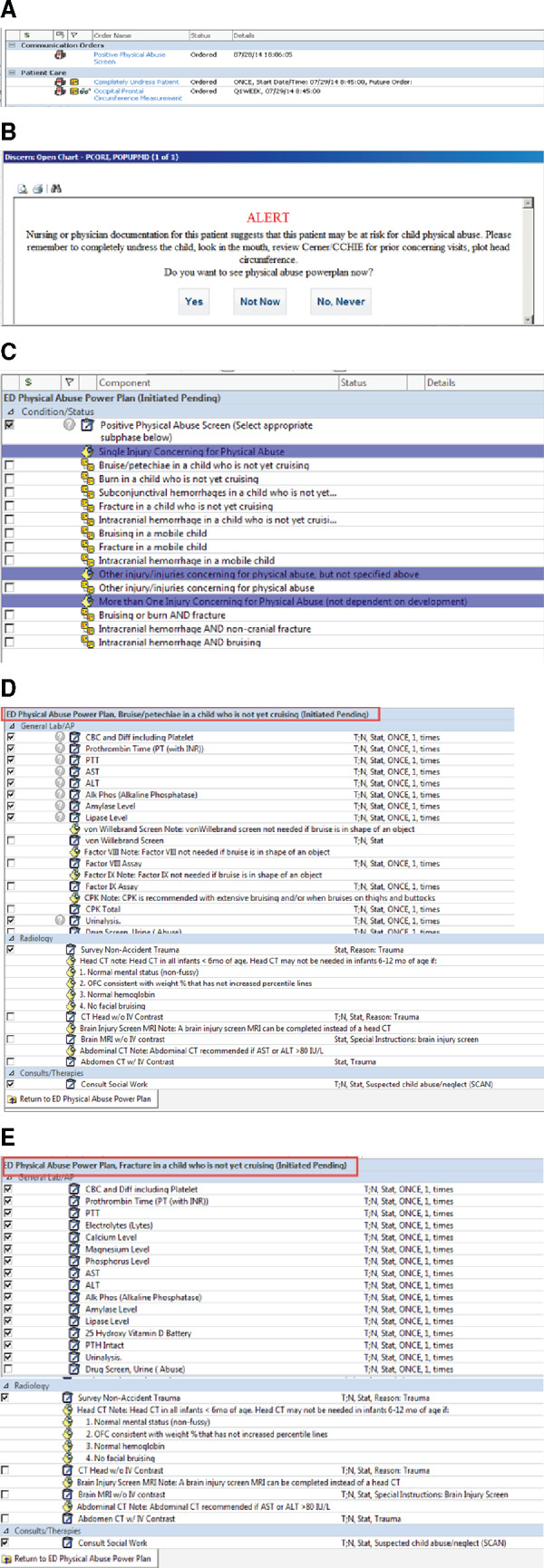
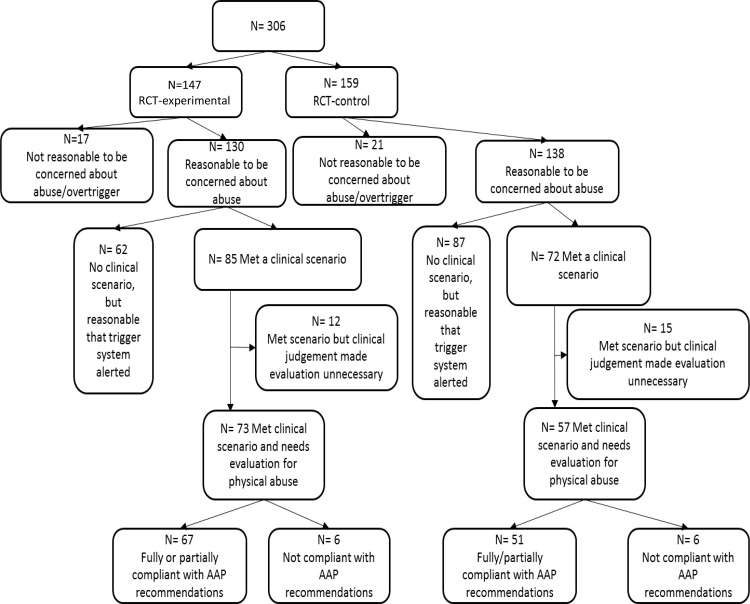
Methods: A randomized controlled trial (RCT) with comparison to a preintervention group was performed. RCT-experimental subjects' providers received alerts with a direct link to a physical abuse-specific order set. RCT-control subjects' providers had no alerts, but could manually search for the order set. Preintervention subjects' providers had neither alerts nor access to the order set. Compliance with clinical guidelines was calculated.
Results: Ninety-nine preintervention subjects and 130 RCT subjects (73 RCT-experimental and 57 RCT-control) met criteria to undergo a physical abuse evaluation. Full compliance with clinical guidelines was 84% pre-intervention, 86% in RCT-control group, and 89% in RCT-experimental group. The physical abuse order set was used 43 times during the 7-month RCT. When the abuse order set was used, full compliance was 100%. The proportion of cases in which there was partial compliance decreased from 10% to 3% once the order set became available (P = .04). Male gender, having >10 years of experience and completion of a pediatric emergency medicine fellowship were associated with increased compliance.
Discussion/conclusion: A child abuse clinical decision support system comprised of a trigger system, alerts and a physical abuse order set was quickly accepted into clinical practice. Use of the physical abuse order set always resulted in full compliance with clinical guidelines. Given the high baseline compliance at our site, evaluation of this alert system in hospitals with lower baseline compliance rates will be more valuable in assessing the efficacy in adherence to clinical guidelines for the evaluation of suspected child abuse.
Figures
References
-
- American Cancer Society. Cancer in Children. 2012. http://www.cancer.org/Cancer/CancerinChildren/DetailedGuide/cancer-in-ch.... Accessed June 5, 2012.
-
- Jenny C, Hymel KP, Ritzen A et al. Analysis of missed cases of abusive head trauma. JAMA 1999;2817:621–626. - PubMed
-
- Ravichandiran N, Schuh S, Bejuk M et al. Delayed identification of pediatric abuse-related fractures. Pediatrics 2010;1251:60–66. - PubMed
-
- King WK, Kiesel EL, Simon HK. Child abuse fatalities: are we missing opportunities for intervention? Pediatr Emerg Care 2006;224:211–214. - PubMed
-
- Pierce MC, Smith S, Kaczor K. Bruising in infants: those with a bruise may be abused. Pediatr Emerg Care. 2009;2512:845–847. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
