

Anti-Ebola Virus Antibody Levels in Convalescent Plasma and Viral Load After Plasma Infusion in Patients With Ebola Virus Disease
- PMID: 29659889
- PMCID: PMC6927845
- DOI: 10.1093/infdis/jiy199
Anti-Ebola Virus Antibody Levels in Convalescent Plasma and Viral Load After Plasma Infusion in Patients With Ebola Virus Disease
Abstract
Background: Ebola virus (EBOV) neutralizing antibody in plasma may reduce viral load following administration of plasma to patients with Ebola virus disease (EVD), but measurement of these antibodies is complex.
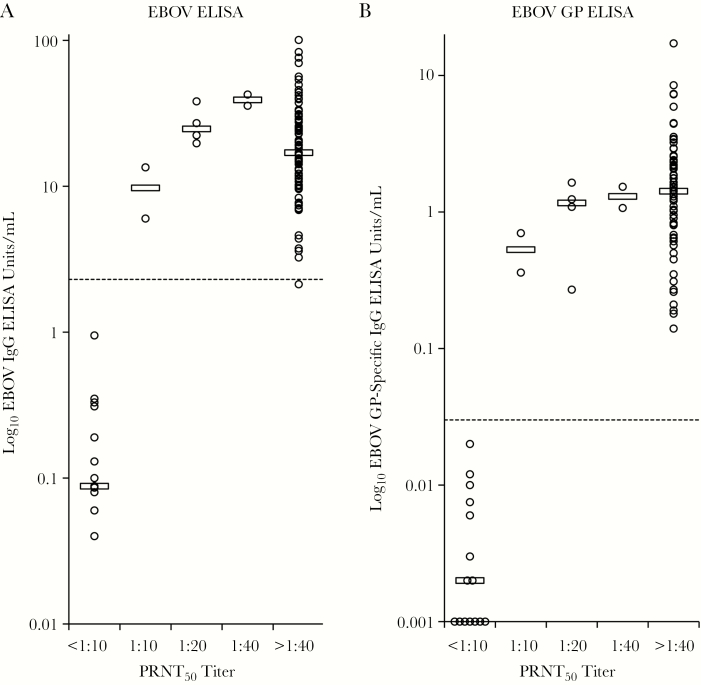
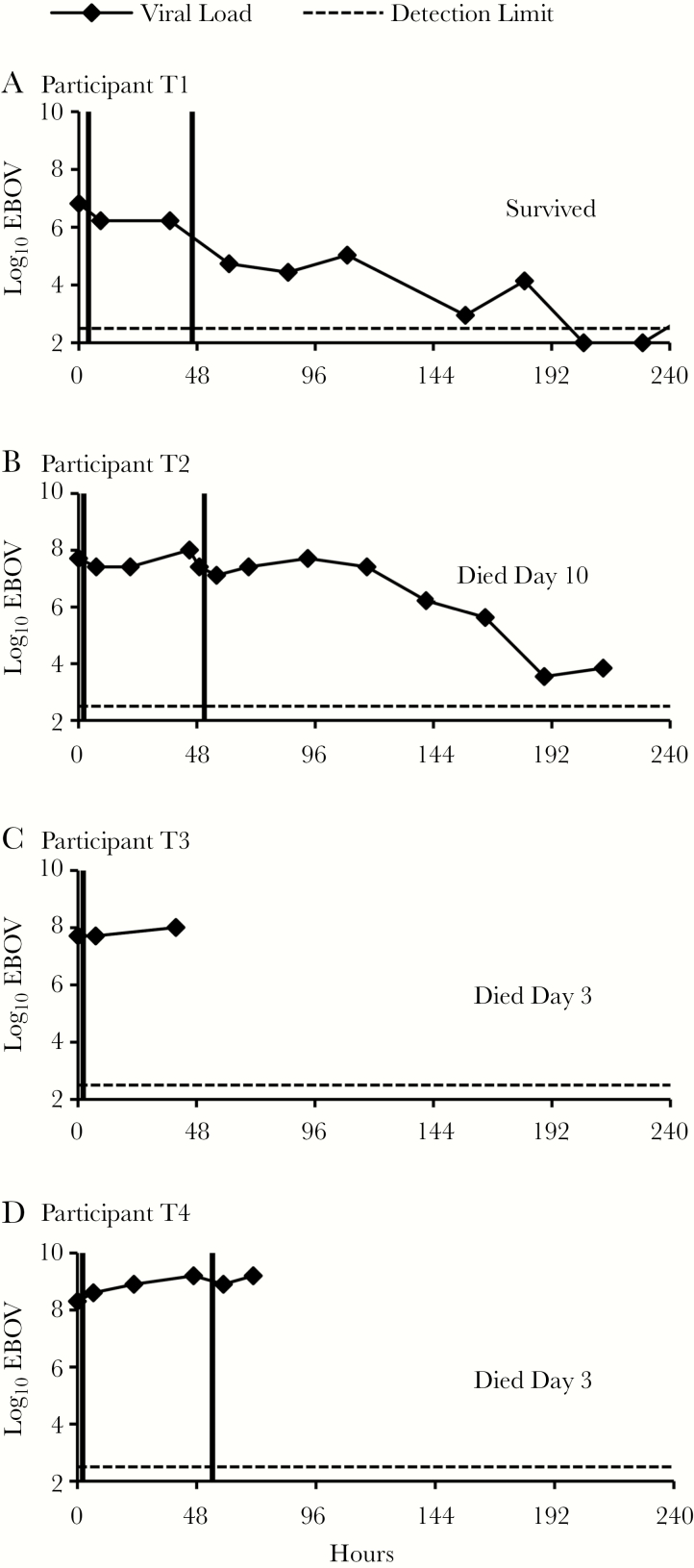
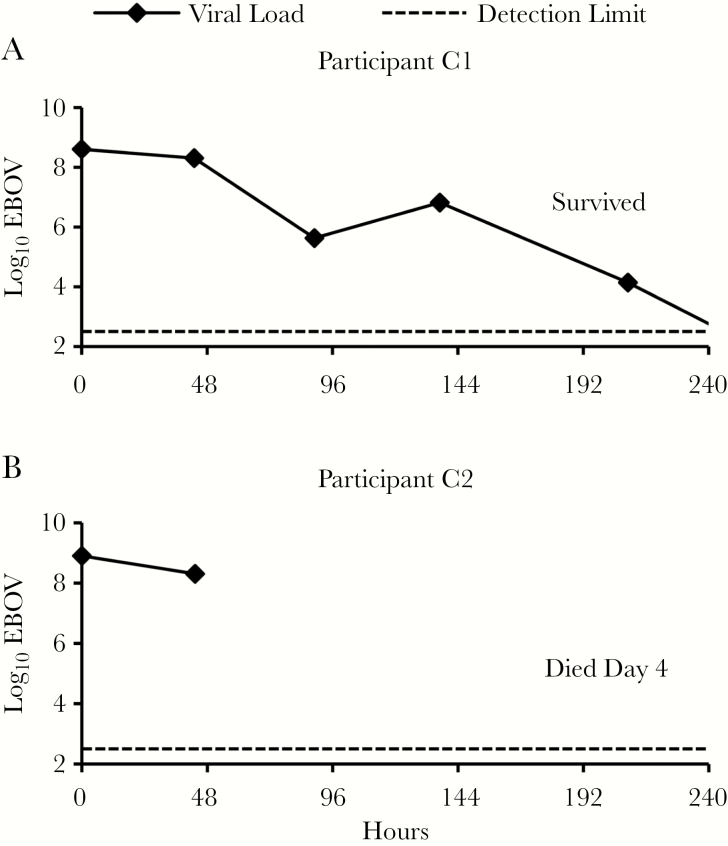
Methods: Anti-EBOV antibody was measured by 2 neutralization and 2 enzyme-linked immunosorbent assays (ELISAs) in convalescent plasma (ECP) from 100 EVD survivor donors in Liberia. Viral load was assessed repetitively in patients with EVD participating in a clinical trial of enhanced standard of care plus ECP.
Results: All 4 anti-EBOV assays were highly concordant for detection of EBOV antibody. Antibodies were not detected in plasma specimens obtained from 15 of 100 donors, including 7 with documented EBOV-positive reverse-transcription polymerase chain reaction during EVD. Viral load was reduced following each dose in the 2 clinical trial participants who received ECP with higher antibody levels but not in the 2 who received ECP with lower antibody levels.
Conclusions: Recovery from EVD can occur with absence of detectable anti-EBOV antibody several months after disease onset. ELISAs may be useful to select ECP donors or identify ECP units that contain neutralizing antibody. ECP with higher anti-EBOV antibody levels may have greater effect on EBOV load-an observation that requires further investigation.
Clinical trials registration: NCT02333578.
Figures
References
-
- Baize S, Leroy EM, Georges-Courbot MC, et al. Defective humoral responses and extensive intravascular apoptosis are associated with fatal outcome in Ebola virus-infected patients. Nat Med 1999; 5:423–6. - PubMed
-
- Surgenor DM, Chalmers TC, Conrad ME, et al. Clinical trials of hepatitis B immune globulin. Development of policies and materials for the 1972-1975 studies sponsored by the National Heart and Lung Institute. N Engl J Med 1975; 293:1060–2. - PubMed
-
- Luke TC, Kilbane EM, Jackson JL, Hoffman SL. Meta-analysis: convalescent blood products for Spanish influenza pneumonia: a future H5N1 treatment?Ann Intern Med 2006; 145:599–609. - PubMed
-
- Maiztegui JI, Fernandez NJ, de Damilano AJ. Efficacy of immune plasma in treatment of Argentine haemorrhagic fever and association between treatment and a late neurological syndrome. Lancet 1979; 2:1216–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
