

Increased Chromogranin A-Positive Hormone-Negative Cells in Chronic Pancreatitis
- PMID: 29659906
- PMCID: PMC6456995
- DOI: 10.1210/jc.2017-01562
Increased Chromogranin A-Positive Hormone-Negative Cells in Chronic Pancreatitis
Abstract
Context: Chronic pancreatitis (CP) is characterized by inflammation, fibrosis, and a loss of pancreatic acinar cells, which can result in exocrine and eventually endocrine deficiency. Pancreatitis has been reported to induce formation of new endocrine cells (neogenesis) in mice. Our recent data have implicated chromogranin A-positive hormone-negative (CPHN) cells as potential evidence of neogenesis in humans.
Objective: We sought to establish if CPHN cells were more abundant in CP in humans.
Design, setting, and participants: We investigated the frequency and distribution of CPHN cells and the expression of the chemokine C-X-C motif ligand 10 (CXCL10) and its receptor chemokine C-X-C motif receptor 3 in pancreas of nondiabetic subjects with CP.
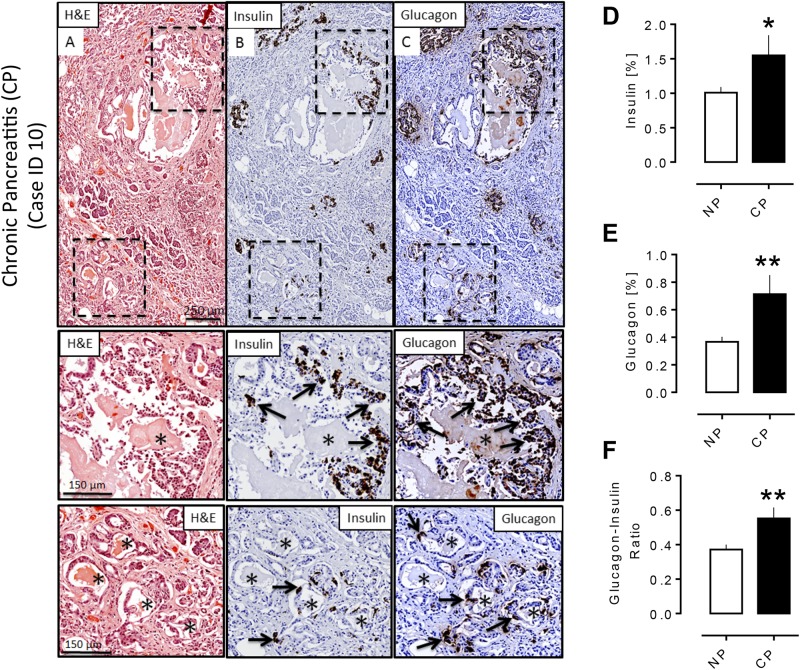
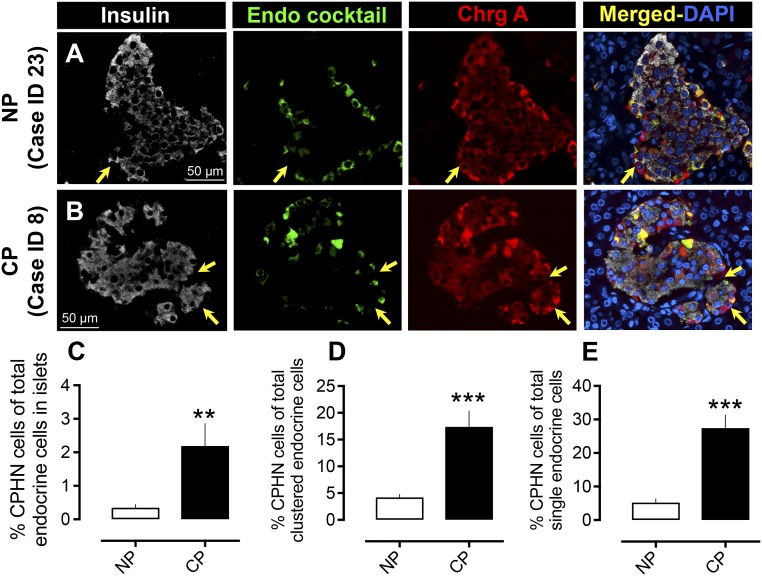
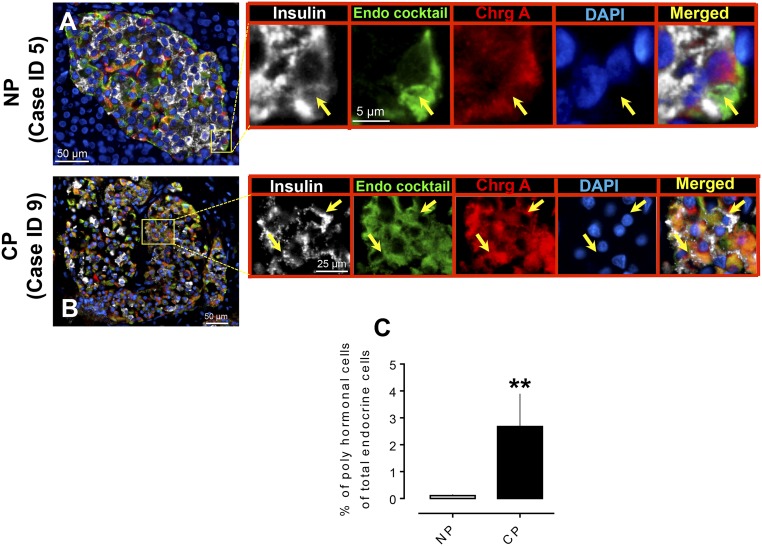
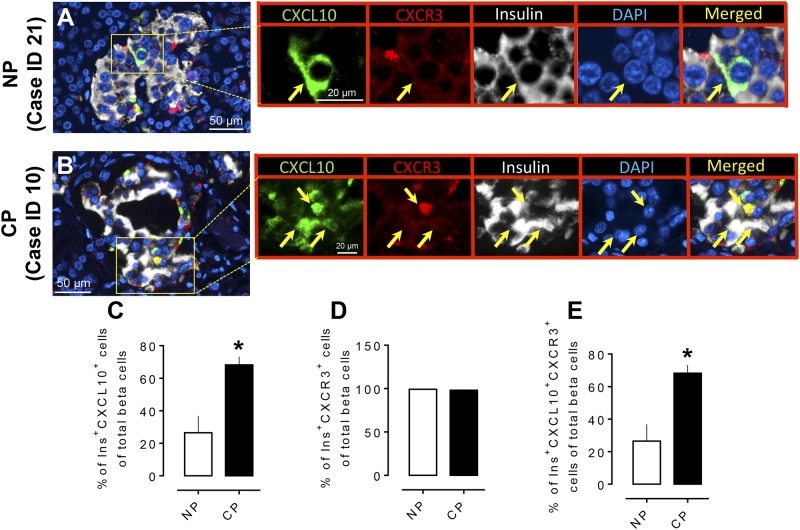
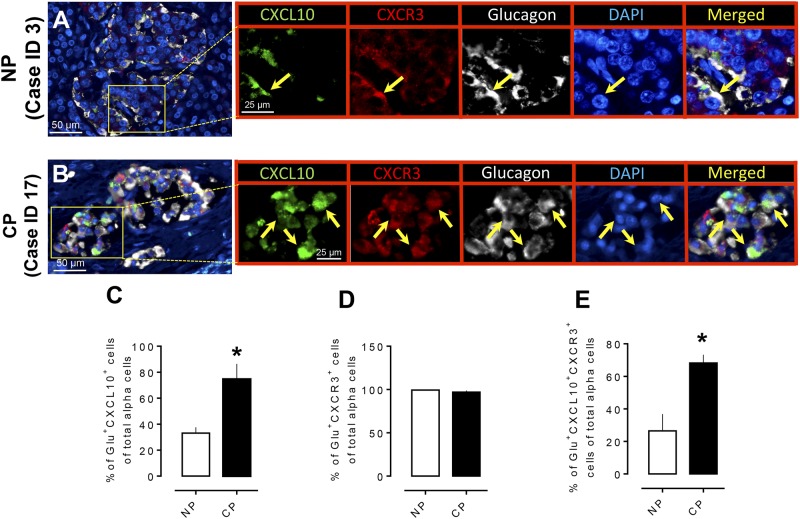
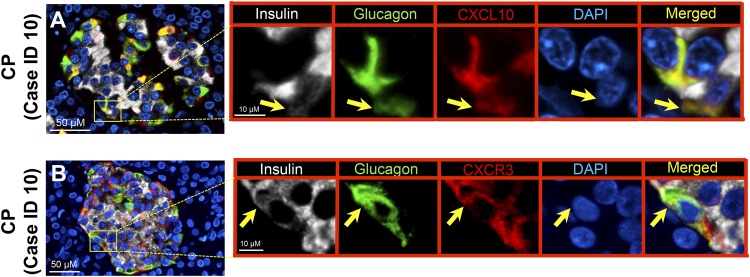
Results: CPHN cell frequency in islets was increased sevenfold in CP [2.1% ± 0.67% vs 0.35% ± 0.09% CPHN cells in islets, CP vs nonpancreatitis (NP), P < 0.01], as were the CPHN cells found as scattered cells in the exocrine areas (17.4 ± 2.9 vs 4.2 ± 0.6, CP vs NP, P < 0.001). Polyhormonal endocrine cells were also increased in CP (2.7 ± 1.2 vs 0.1 ± 0.04, CP vs NP, % of polyhormonal cells of total endocrine cells, P < 0.01), as was expression of CXCL10 in α and β cells.
Conclusion: There is increased islet endogenous expression of the inflammation marker CXCL10 in islets in the setting of nondiabetic CP and an increase in polyhormonal (insulin-glucagon expressing) cells. The increase in CPHN cells in CP, often in a lobular distribution, may indicate foci of attempted endocrine cell regeneration.
Figures
References
-
- Klöppel G, Maillet B. The morphological basis for the evolution of acute pancreatitis into chronic pancreatitis. Virchows Arch A Pathol Anat Histopathol. 1992;420(1):1–4. - PubMed
-
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med. 1995;332(22):1482–1490. - PubMed
-
- Lankisch PG, Löhr-Happe A, Otto J, Creutzfeldt W. Natural course in chronic pancreatitis: pain, exocrine and endocrine pancreatic insufficiency and prognosis of the disease. Digestion. 1993;54(3):148–155. - PubMed
-
- Ammann RW, Akovbiantz A, Largiader F, Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 245 patients. Gastroenterology. 1984;86(5 Pt 1):820–828. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
