

Metastases in Prostate Cancer
- PMID: 29661810
- PMCID: PMC6396340
- DOI: 10.1101/cshperspect.a033688
Metastases in Prostate Cancer
Erratum in
-
Erratum: Metastases in Prostate Cancer.Cold Spring Harb Perspect Med. 2018 Jul 2;8(7):a035568. doi: 10.1101/cshperspect.a035568. Cold Spring Harb Perspect Med. 2018. PMID: 29967098 Free PMC article. No abstract available.
Abstract
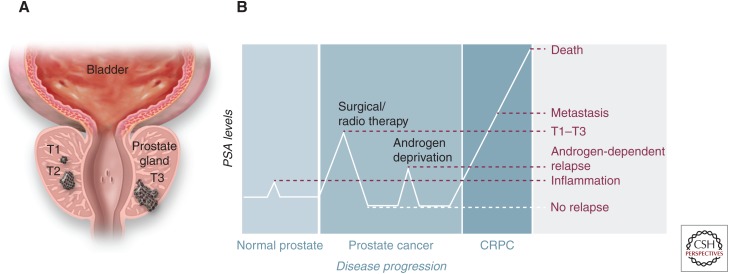
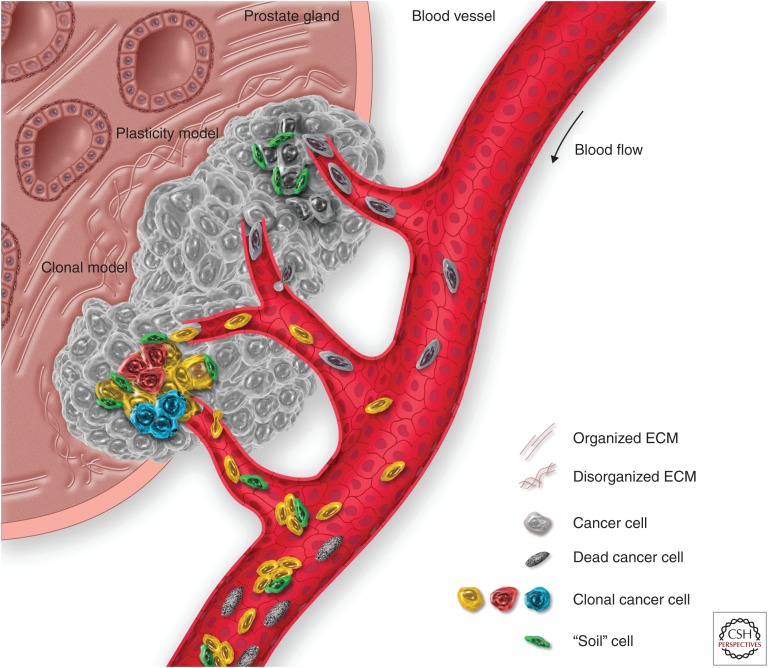
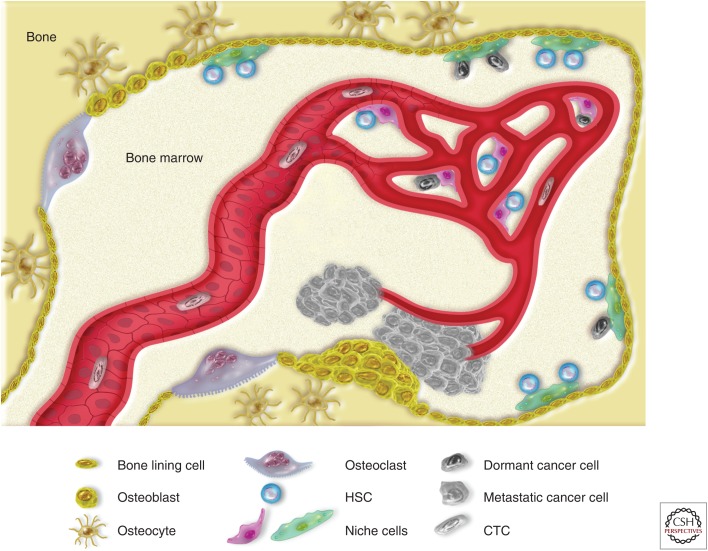
Prostate cancer (PCa) prognosis and clinical outcome is directly dependent on metastatic occurrence. The bone microenvironment is a favorable metastatic niche. Different biological processes have been suggested to contribute to the osteotropism of PCa such as hemodynamics, bone-specific signaling interactions, and the "seed and soil" hypothesis. However, prevalence of disseminating tumor cells in the bone is not proportional to the actual occurrence of metastases, as not all patients will develop bone metastases. The fate and tumor-reforming ability of a metastatic cell is greatly influenced by the microenvironment. In this review, the molecular mechanisms of bone and soft-tissue metastasis in PCa are discussed. Specific attention is dedicated to the residual disease, novel approaches, and animal models used in oncological translational research are illustrated.
Copyright © 2019 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
References
-
- Adsan Ö, Cecchini MG, Bisoffi M, Wetterwald A, Klima I, Danuser HJ, Studer UE, Thalmann GN. 2002. Can the reverse transcriptase-polymerase chain reaction for prostate specific antigen and prostate specific membrane antigen improve staging and predict biochemical recurrence? BJU Int 90: 579–585. - PubMed
-
- Arai F, Hirao A, Ohmura M, Sato H, Matsuoka S, Takubo K, Ito K, Koh GY, Suda T. 2004. Tie2/Angiopoietin-1 signaling regulates hematopoietic stem cell quiescence in the bone marrow niche. Cell 118: 149–161. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical