

Characterization of Extensively Drug-Resistant or Pandrug-Resistant Sequence Type 147 and 101 OXA-48-Producing Klebsiella pneumoniae Causing Bloodstream Infections in Patients in an Intensive Care Unit
- PMID: 29661874
- PMCID: PMC6021667
- DOI: 10.1128/AAC.02457-17
Characterization of Extensively Drug-Resistant or Pandrug-Resistant Sequence Type 147 and 101 OXA-48-Producing Klebsiella pneumoniae Causing Bloodstream Infections in Patients in an Intensive Care Unit
Abstract
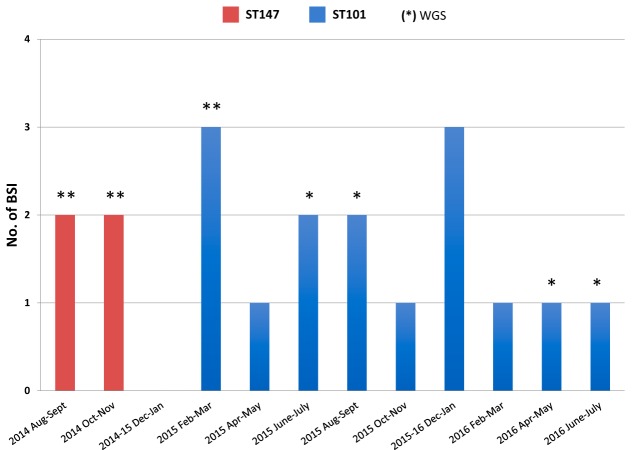
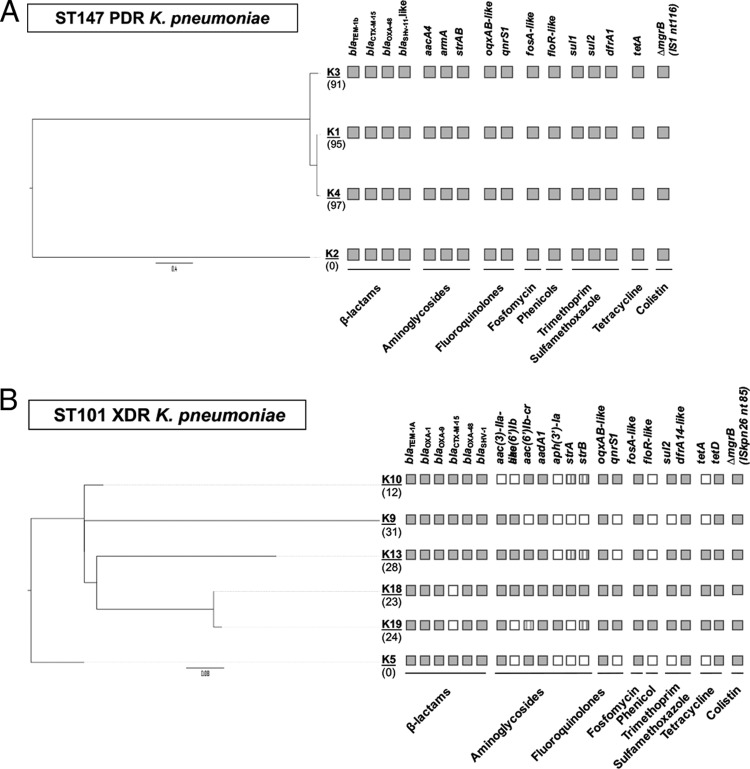
Carbapenem-resistant Klebsiella pneumoniae causes important health care-associated infections worldwide. An outbreak of sequence type 11 (ST11) OXA-48-producing K. pneumoniae (OXA-48-Kp) isolates occurred in Tzaneio Hospital in 2012 and was contained until 2014, when OXA-48-Kp reemerged. The present study involved 19 bloodstream infection (BSI) OXA-48-Kp isolates recovered from 19 intensive care unit (ICU) patients hospitalized between August 2014 and July 2016. MICs were determined by broth microdilution. Beta-lactamase genes were detected by PCR. All isolates were typed by pulsed-field gel electrophoresis/multilocus sequence typing (PFGE/MLST), and 10 representative isolates were typed by next-generation sequencing (NGS). Of the 19 study patients, 9 had previous hospitalizations, and 10 carried OXA-48-Kp prior to BSI isolation; median time from ICU admission to BSI was 29 days. Four OXA-48-Kp isolates belonged to PFGE profile A (ST147) and were pandrug resistant (PDR), while 15 isolates exhibited PFGE profile B (ST101) and were extensively drug resistant. Genes detected via NGS resistome analysis accounted for most of the resistance phenotypes, except for tigecycline and fosfomycin. Insertional inactivation of mgrB (distinct per clone) conferred colistin resistance in all 19 isolates. NGS single nucleotide polymorphism (SNP) analysis validated the clonal relatedness of the ST147 and ST101 strains and revealed the possible presence of two index ST147 strains and the microevolution of ST101 strains. Distinct, but highly related, IncL OXA-48-encoding plasmid lineages were identified; plasmids of the ST147 strains were identical with the plasmid of ST11 OXA-48-Kp which caused the 2012 outbreak. In conclusion, biclonal circulation of OXA-48-Kp and, alarmingly, emergence of a PDR clone are reported. These observations, along with the challenging phenotypic detection of OXA-48 producers and the high reported transmissibility of blaOXA-48, necessitate intensive efforts to prevent their further spread.
Keywords: NGS; SNPs; biclonal circulation; carbapenemases; microevolution.
Copyright © 2018 American Society for Microbiology.
Figures
References
-
- Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, Cormican M, Cornaglia G, Garau J, Gniadkowski M, Hayden MK, Kumarasamy K, Livermore DM, Maya JJ, Nordmann P, Patel JB, Paterson DL, Pitout J, Villegas MV, Wang H, Woodford N, Quinn JP. 2013. Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. Lancet Infect Dis 13:785–796. doi: 10.1016/S1473-3099(13)70190-7. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
