

Association between Loss of Skeletal Muscle Mass and Mortality and Tumor Recurrence in Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 29662836
- PMCID: PMC5892377
- DOI: 10.1159/000484950
Association between Loss of Skeletal Muscle Mass and Mortality and Tumor Recurrence in Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Abstract
Background: Hepatocellular carcinoma (HCC) has multiple prognostic factors, and there is an increase in knowledge about the body composition and physical status of patients with HCC. The present meta-analysis aimed to explore whether loss of skeletal muscle mass is associated with mortality and tumor recurrence in patients with HCC.
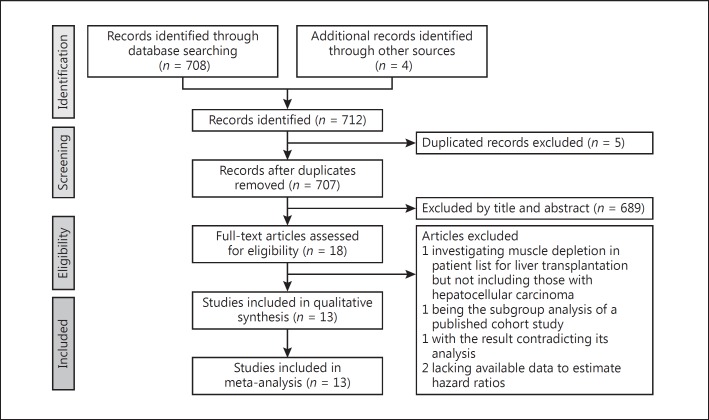
Method: A systematic search was conducted for published literature using PubMed, Embase, and Scopus. We included cohort or case-control studies investigating patients with HCC. The primary and secondary outcomes were the associations of loss of skeletal muscle mass with overall survival and tumor recurrence, respectively, expressed by a summary hazard ratio (HR) and 95% confidence interval (CI).
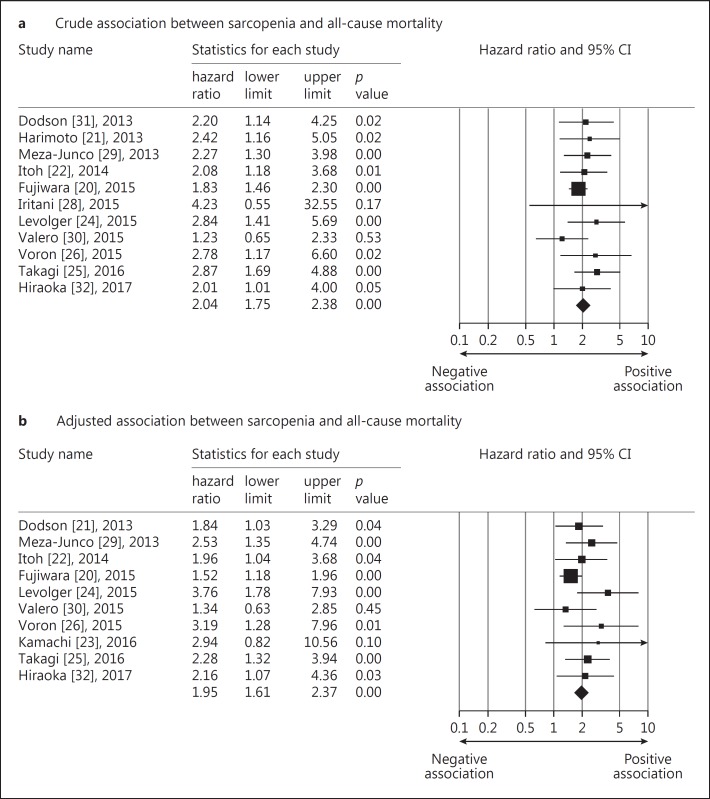
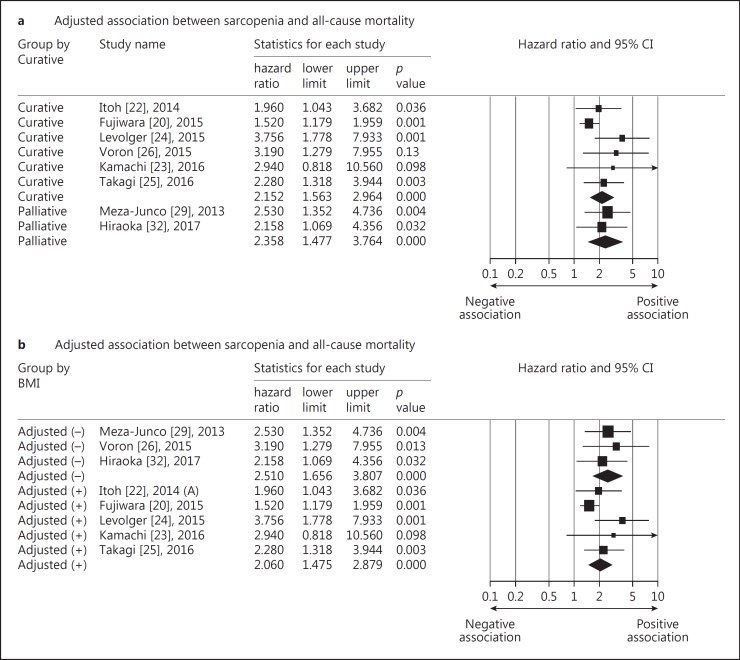
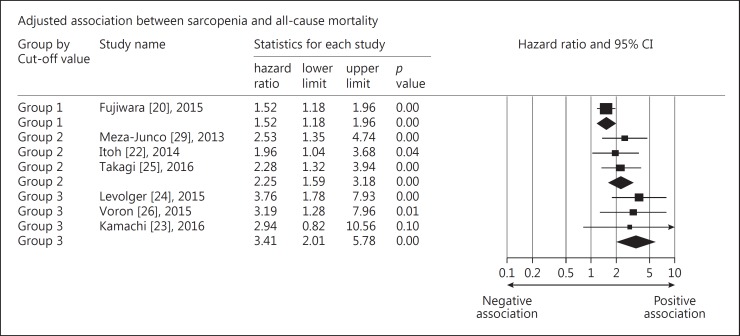
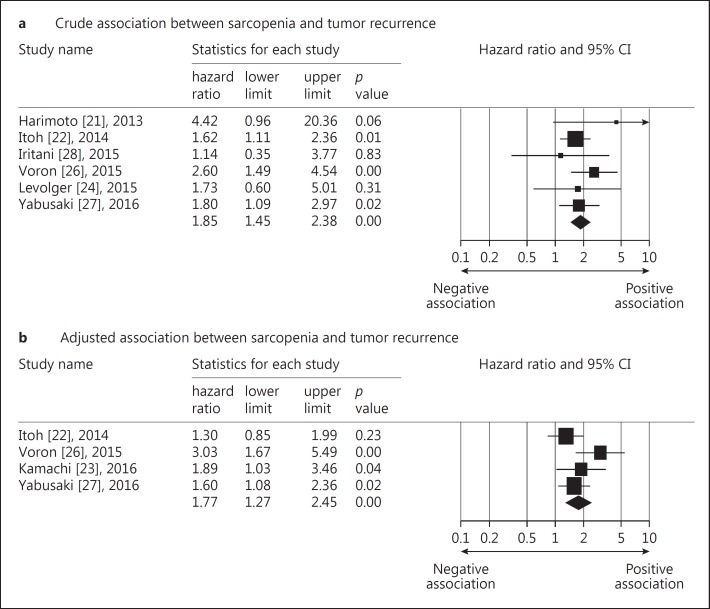
Result: A total of 13 studies comprising 3,111 patients were included. The summary HRs calculated by either univariate or multivariate analysis both suggested a significant association between sarcopenia and all-cause mortality (crude HR = 2.04, 95% CI: 1.74-2.38; adjusted HR = 1.95, 95% CI: 1.60-2.37). Similarly, loss of skeletal muscle mass was associated with tumor recurrence (crude HR = 1.85, 95% CI: 1.44-2.37; adjusted HR = 1.76, 95% CI: 1.27-2.45). The stratified analysis showed that treatment types and inclusion of body mass index or body weight in the Cox regression model did not modify both clinical outcomes. With an increase in cut-off values of muscle mass on computed tomography images (especially for male patients), there was an insignificant trend of stronger associations between loss of skeletal muscle mass and all-cause mortality.
Conclusion: Loss of skeletal muscle mass is associated with increased all-cause mortality and tumor recurrence in patients with HCC. Further prospective studies incorporating measurements of muscle strength and physical function are warranted to see whether inclusion of both parameters better predicts the outcome than use of muscle mass only.
Keywords: Cancer; Hepatocellular carcinoma; Muscle mass; Sarcopenia; Survival.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
