

Review
doi: 10.1155/2018/9608947.
eCollection 2018.
Demystifying MR Neurography of the Lumbosacral Plexus: From Protocols to Pathologies
Affiliations
- PMID: 29662907
- PMCID: PMC5832061
- DOI: 10.1155/2018/9608947
Item in Clipboard
Review
Demystifying MR Neurography of the Lumbosacral Plexus: From Protocols to Pathologies
Biomed Res Int.
.
Abstract
Magnetic resonance neurography is a high-resolution imaging technique that allows evaluating different neurological pathologies in correlation to clinical and the electrophysiological data. The aim of this article is to present a review on the anatomy of the lumbosacral plexus nerves, along with imaging protocols, interpretation pitfalls, and most common pathologies that should be recognized by the radiologist: traumatic, iatrogenic, entrapment, tumoral, infectious, and inflammatory conditions. An extensive series of clinical and imaging cases is presented to illustrate key-points throughout the article.
Figures

Illustrations ((a) and (b)) showing the anatomy of the lumbar plexus, which is formed by the ventral rami of L1–L4 ± T12, gathering inside or posterior to the psoas muscle belly. The lumbar plexus originates from the iliohypogastric nerves (T12 ± L1), ilioinguinal (L1 ± T12), genitofemoral (L1 and L2), femoral (L2–L4), cutaneous femoral (L2 and L3), obturator (L2–L4), and lumbosacral trunk (L4 and L5). ∗Illustrations by FJMN.

MR images in coronal STIR 3D SPACE (MIP) in (a), showing nerve roots of the lumbar plexus (L1 to L4) and the femoral nerve, formed by posterior nerve roots from L2 to L4, emerging lateral to the psoas muscle. In (b), MR images show L5 and S1 nerve roots, the lumbosacral trunk formed by the anastomotic branches of L4 and L5 nerve roots, and the sciatic nerve formed by major branches of the sacral plexus from L4 to S3.

34-year-old male with history of thigh pain 1 month ago. MRN images in coronal T2 (a), axial diffusion-weighted imaging (b), axial T2 fat suppression (c), and T1 postcontrast (d) show signal change with slight thickening and contrast enhancement of the left lateral cutaneous nerve (solid arrow), predominating at the level of the fibrous tunnel underlying the inguinal ligament and iliac crest (arrowhead), representing neuritis.

53-year-old male subject, with history of falling to the ground, presenting weakness in the right lower limb and with drop foot on physical examination. MRN images in coronal STIR 3D SPACE (a) and coronal T2 with fat suppression (b) of the right hip show slight thickening and elevation of signal intensity in the sciatic nerve (solid arrows) from its origin in the lumbosacral plexus to the thigh (neural stretching). MRN images in coronal STIR 3D SPACE (c) demonstrate lumbar plexus trunk thickening (arrowhead). MRN images in axial T2 (d) show diffuse edema affecting the tensor of fascia lata muscle (wavy arrow) and gluteus minimus (star), compatible with acute denervation/neuropathy.

34-year-old male with history of chronic pain after traumatic injury in motorcycle accident for 2 months with surgery on the femur with plaque placement. MRN images in coronal STIR 3D SPACE ((a) and (b)) and axial T2 fat suppression (c) show signs of right femoral neuropathy, with thickening and elevation of the femoral nerve signal in the retroperitoneal and proximal thigh trajectory (arrowhead). Early stage denervation is associated with edema and a slight contrast enhancement of the distal iliopsoas (star) and pectineus (wavy arrow) muscles.
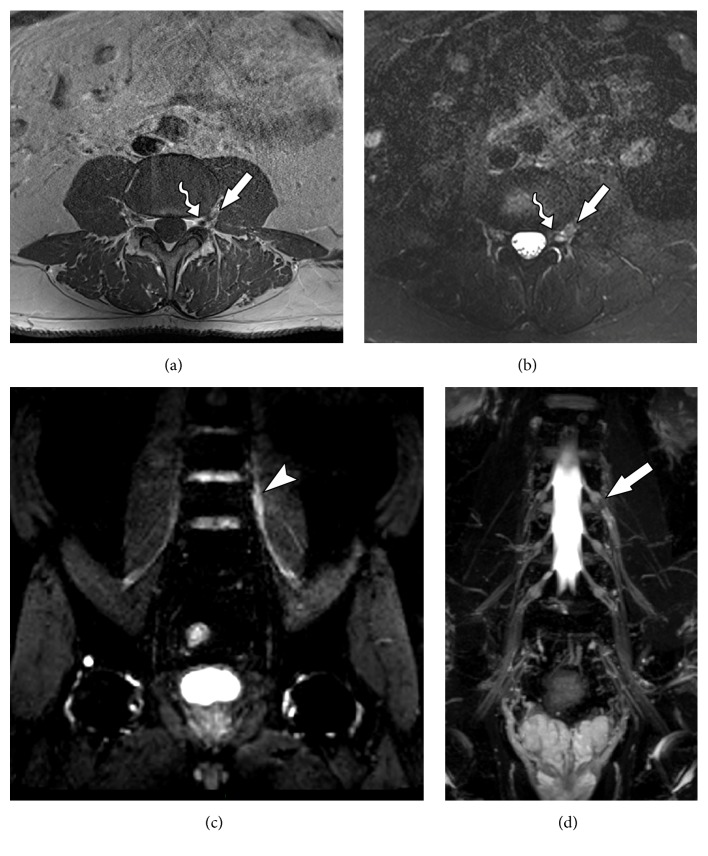
65-year-old male admitted to the emergency room with history of sudden low back pain radiating to the left lower limb. MRN images in axial T1 (a), axial T2 fat suppression (b), coronal diffusion-weighted imaging (c), and coronal diffusion-weighted imaging MPR reconstruction (d) show left foraminal/extreme lateral discal hernia in L3-L4 level, with extruded discal fragment (solid arrow) compressing the left L3 nerve root (wavy arrow) along its emergence. Slight thickening is associated in the proximal segment, as well as T2 hyperintensity and diffusion restriction (arrowhead).

34-year-old male with history of left hip pain with radiation to lower left limb after soccer training. MRN images in axial T1 (a), axial T2 fat suppression (b), coronal T2 3D SPACE (c), and coronal STIR 3D SPACE (d) show a heterogeneous tissue (solid arrow) with high intensity in T2, with low signal foci in perineural region posterior to the left L5 nerve root (wavy arrow) anteriorly to the left sacral wing. There is thickening and abnormal signal intensity of the left nerve root of L5 (arrowhead), as well as of fascicles of the nerve to the proximal thigh segment, with a high T2 signal and postcontrast enhancement (neuropathy). The appearance is compatible with L5-S1 left extraforaminal disc extrusion material, with extensive lower migration and neural compression.

31-year-old female subject, presenting numbness and tingling on the left lower extremity for three months. Past medical history of endometriosis. MRN images on axial T2 isotropic (a), coronal T2 isotropic (b), axial T1 VIBE subtraction (c) show deep endometriosis in the uterine retrocervical region, extending to the left paracervical space maintaining an intimate relationship with the pelvic root path (solid arrows) and axial T2 FLAIR (d) demonstrates slight change of the emerging left S2 root signal intensity with mild contrast enhancement (arrowhead).

38-year-old male with history of neurofibromatosis with low back pain. MRN images in coronal STIR 3D SPACE MIP (a), sagittal STIR 3D SPACE (b), and axial STIR 3D SPACE (c) and axial T1 VIBE postcontrast show multiple small nodular images (arrowhead) in the neural roots of the lumbosacral plexus, with bilateral nodular thickening measuring up to 2 cm, extending from the emergencies to the sciatic nerves. Compatible with neurofibromas in the clinical setting. Two major nodular lesions with well-defined contours, one in the left lateral topography of the aortic bifurcation (star) and the other in left perirectal topography (wavy arrow) that may represent neurofibromas with degeneration.

73-year-old female with pain for 4 months in sciatic territory, with history of Hodgkin lymphoma undergoing chemotherapy. MRN images in axial T1-weighted contrast-enhanced (a), coronal VIBE subtraction (b), and coronal T1 postcontrast VIBE 3D SPACE ((c) and (d)) show a large, lobular, contrasting, infiltrative mass (solid arrows) suggestive of a lymphoproliferative process, disseminated inferiorly through the left paravertebral region near the psoas and presacral region. The mass also infiltrates the left neural foramina and emergent nerve roots of L4-L5 and L5-S1 and, bilaterally, in S1-S2 to S4-S5. It determines diffuse involvement of the left sacral plexus, proximal segments of the obturator, pudendal and sciatic nerve, close to the piriformis and internal obturator muscles (arrowhead). There is also signs of bone infiltration (wavy arrow).

73-years old male with history of weakness and paresthesia in the lower left limb. Previous history of left nephrectomy due to renal tumor 5 years ago. MRN images on coronal T2 3D isotropic (a), axial T2 (b), axial T2 with fat suppression (c) and axial axial T1-weighted contrast-enhanced (d) showing a solid tissue and neural thickening of the proximal sciatic plexus, with contrast enhancement (solid arrow) and cystic areas of permeation (arrowhead), characterizing neoplastic infiltration.

48-years female smoker with lung cancer developing lumbar and right limb pain. MRN images in axial T1 (a), axial T2 fat suppression (b), axial T1 VIBE post contrast (c) and coronal STIR 3D SPACE MIP (d) show a large right hip mass (solid arrow) with soft tissue components and necrosis associated with edema and enhancement of adjacent soft tissues (arrowhead). The inflammatory process involves the sciatic nerve (wavy arrow), with thickening and contrast enhancement. Femoral neuropathy is also seen (star).

74-years male with low back pain related to a paravertebral tumor. Biopsy revealed an undifferentiated liposarcoma. MRN images in coronal axial T2 (a), sagittal T2 (b), coronal STIR 3D SPACE (c) and coronal STIR 3D SPACE MPR (d) show a heterogeneous solid mass with high T2-weighted signal intensity predominance and contrast enhancement, infiltrating the right psoas muscle in L5 and S1 planes (solid arrow). There is also an extension to the iliac musculature and right lateral aspect of L5 vertebral body, with small insinuation to the neural L5-S1 foramen. The lesion involves the extraforaminal pathway of the L4 root and the proximal portion of the femoral nerve (arrowhead).

43-years male in late postoperative stage of gastroplasty with progressive low back pain and febrile spikes. MRN images in coronal T1 VIBE post contrast (a), axial T1 VIBE post contrast (b), coronal STIR coronal diffusion-weighted (c) and coronal STIR 3D SPACE (d) show fluid collection in the surgical bed at the right iliopsoas muscle, with intense peripheral contrast enhancement (solid arrow). The L3 nerve root (arrowhead) presents signs of neuropathy. The right L4 nerve root (star) emerges through the surgical bed and is also diffusely thickened, with edema and contrast enhancement throughout its course, up to the level of the inguinal region.

83-years male, diabetic patient non-responsive to insulin therapy, presenting chronic pain in the lower limbs. MRN images in coronal STIR 3D SPACE MPR (a), axial T2 fat suppression (b), axial T1 VIBE subtraction (c) and coronal T1 VIBE subtraction (d) show left femoral nerve (solid arrow) thickening with inflammatory signs, throughout from its origin to the thigh, associated to diffuse edema perineural planes. Fluid is seen around the muscle, and along the neural path (star). Obturator nerve (arrowhead) is discretely thickened and with inflammatory signals since its origin to distal portions. These findings are suggestive for inflammatory polyradiculoneuropathy.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
