

Procalcitonin algorithm to guide initial antibiotic therapy in acute exacerbations of COPD admitted to the ICU: a randomized multicenter study
- PMID: 29663044
- PMCID: PMC5924665
- DOI: 10.1007/s00134-018-5141-9
Procalcitonin algorithm to guide initial antibiotic therapy in acute exacerbations of COPD admitted to the ICU: a randomized multicenter study
Abstract
Purpose: To compare the efficacy of an antibiotic protocol guided by serum procalcitonin (PCT) with that of standard antibiotic therapy in severe acute exacerbations of COPD (AECOPDs) admitted to the intensive care unit (ICU).
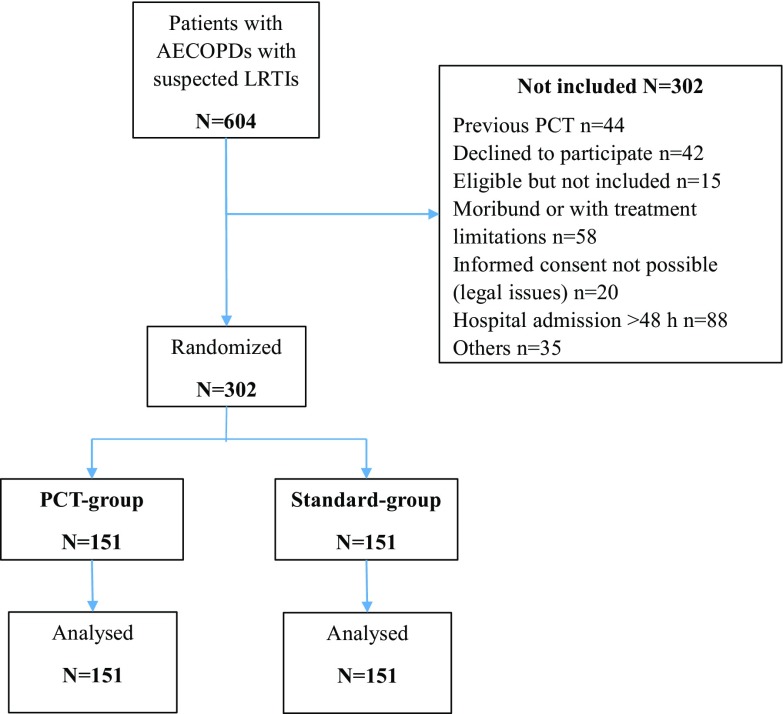
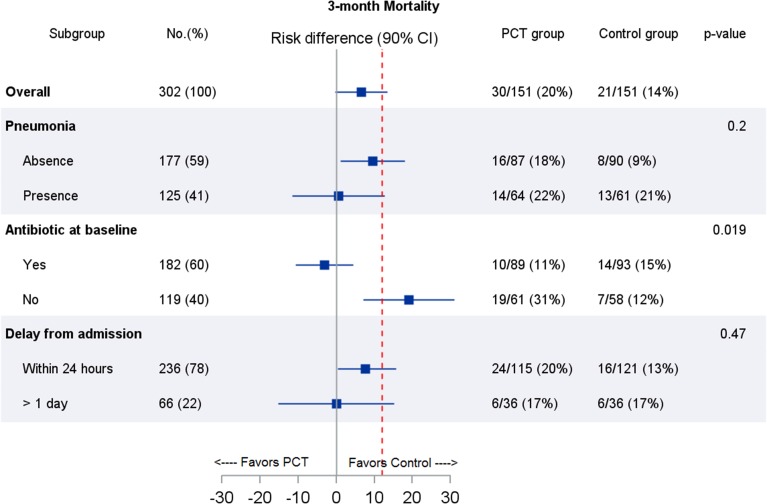
Methods: We conducted a multicenter, randomized trial in France. Patients experiencing severe AECOPDs were assigned to groups whose antibiotic therapy was guided by (1) a 5-day PCT algorithm with predefined cutoff values for the initiation or stoppage of antibiotics (PCT group) or (2) standard guidelines (control group). The primary endpoint was 3-month mortality. The predefined noninferiority margin was 12%.
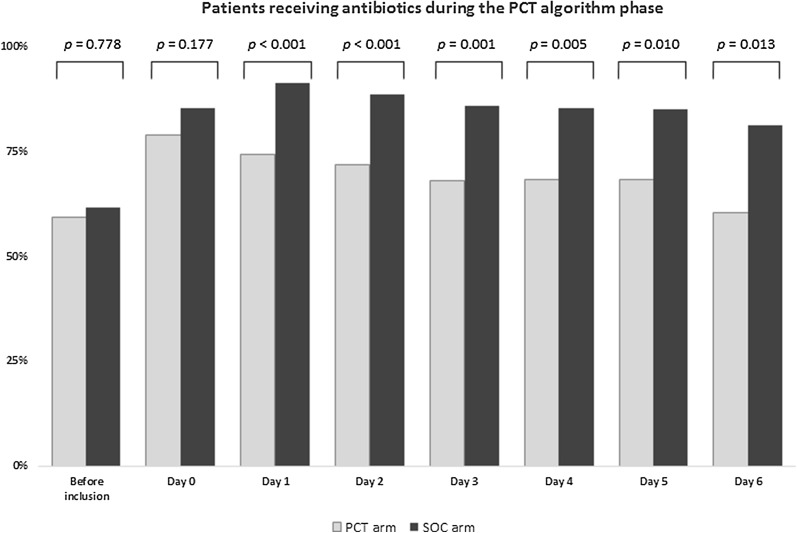
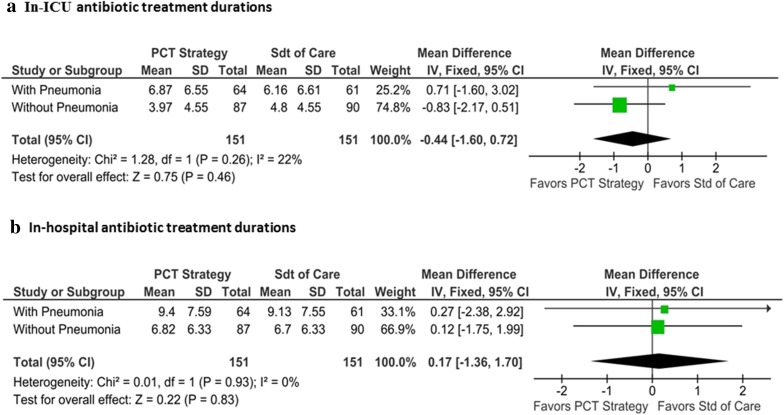
Results: A total of 302 patients were randomized into the PCT (n = 151) and control (n = 151) groups. Thirty patients (20%) in the PCT group and 21 patients (14%) in the control group died within 3 months of admission (adjusted difference, 6.6%; 90% CI - 0.3 to 13.5%). Among patients without antibiotic therapy at baseline (n = 119), the use of PCT significantly increased 3-month mortality [19/61 (31%) vs. 7/58 (12%), p = 0.015]. The in-ICU and in-hospital antibiotic exposure durations, were similar between the PCT and control group (5.2 ± 6.5 days in the PCT group vs. 5.4 ± 4.4 days in the control group, p = 0.85 and 7.9 ± 8 days in the PCT group vs. 7.7 ± 5.7 days in the control group, p = 0.75, respectively).
Conclusion: The PCT group failed to demonstrate non-inferiority with respect to 3-month mortality and failed to reduce in-ICU and in-hospital antibiotic exposure in AECOPDs admitted to the ICU.
Keywords: Antibiotic stewardship; Chronic obstructive pulmonary disease; Community-acquired pneumonia; Procalcitonin; Respiratory tract infection; Viral infection.
Conflict of interest statement
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical approval
The study protocol was approved by the local research ethic committee (Comité de Protection des Personnes Nord Ouest III) for all participating centres.
Informed consent
Written informed consent was obtained from the patients or their surrogates upon their enrolment in the study.
Figures
References
-
- Woodhead M, Blasi F, Ewig S, Garau J, Huchon G, Ieven M, Ortqvist A, Schaberg T, Torres A,, van der Heijden G, Read R, Verheij TJ, Joint Taskforce of the European Respiratory Society and European Society for Clinical Microbiology and Infectious Diseases Guidelines for the management of adult lower respiratory tract infections–full version. Clin Microbiol Infect. 2011;17(Suppl 6):E1–E59. doi: 10.1111/j.1469-0691.2011.03672.x. - DOI - PMC - PubMed
-
- Soler N, Torres A, Ewig S, Gonzalez J, Celis R, El-Ebiary M, Hernandez C, Rodriguez-Roisin R. Bronchial microbial patterns in severe exacerbations of chronic obstructive pulmonary disease (COPD) requiring mechanical ventilation. Am J Respir Crit Care Med. 1998;157:1498–1505. doi: 10.1164/ajrccm.157.5.9711044. - DOI - PubMed
-
- Christ-Crain M, Jaccard-Stolz D, Bingisser R, Gencay MM, Huber PR, Tamm M, Müller B. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet. 2004;363:600–607. doi: 10.1016/S0140-6736(04)15591-8. - DOI - PubMed
-
- Schuetz P, Christ-Crain M, Thomann R, Falconnier C, Wolbers M, Widmer I, Neidert S, Fricker T, Blum C, Schild U, Regez K, Schoenenberger R, Henzen C, Bregenzer T, Hoess C, Krause M, Bucher HC, Zimmerli W, Mueller B. ProHOSP Study Group. Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA. 2009;302:1059–1066. doi: 10.1001/jama.2009.1297. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
