

β-Catenin-mediated immune evasion pathway frequently operates in primary cutaneous melanomas
- PMID: 29664013
- PMCID: PMC5919828
- DOI: 10.1172/JCI95351
β-Catenin-mediated immune evasion pathway frequently operates in primary cutaneous melanomas
Abstract
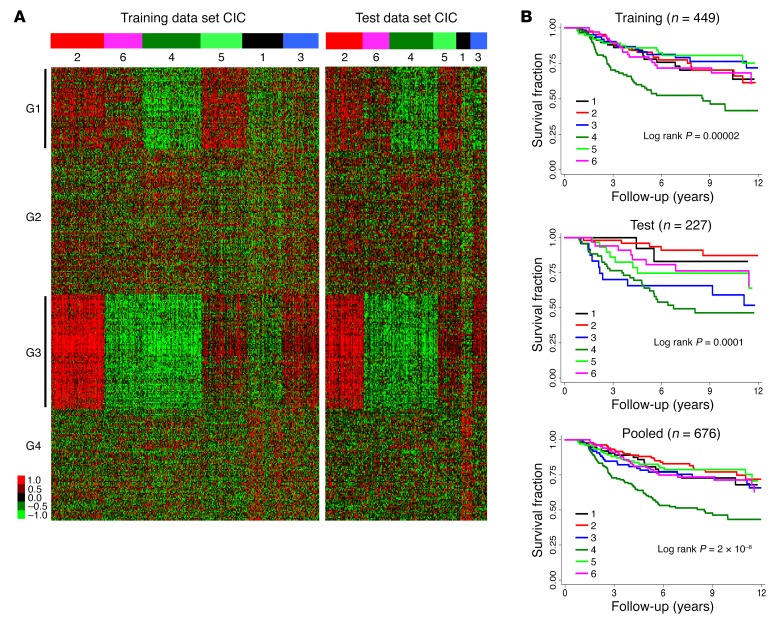
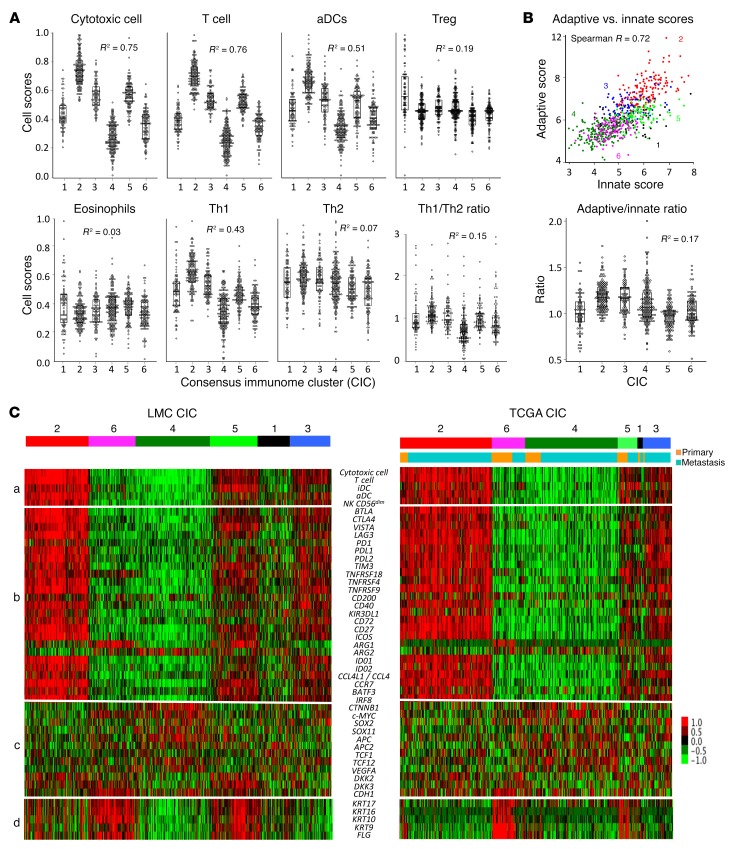
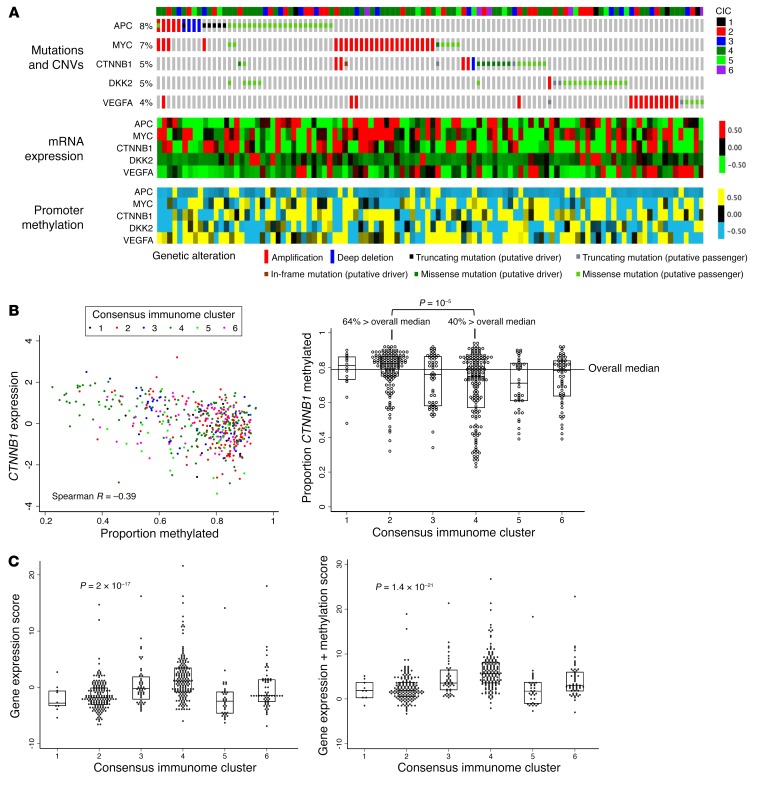
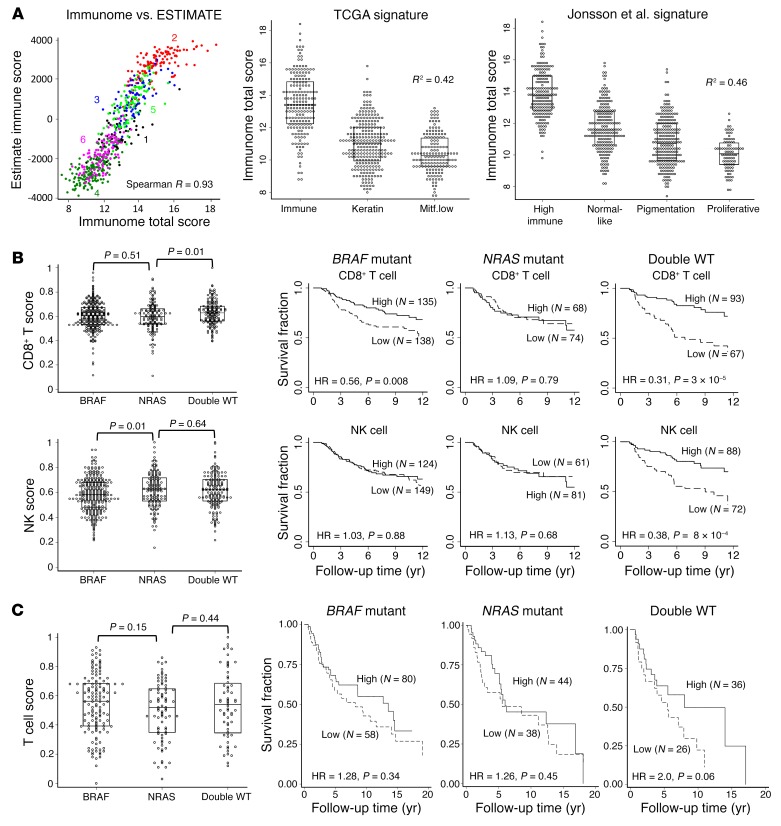
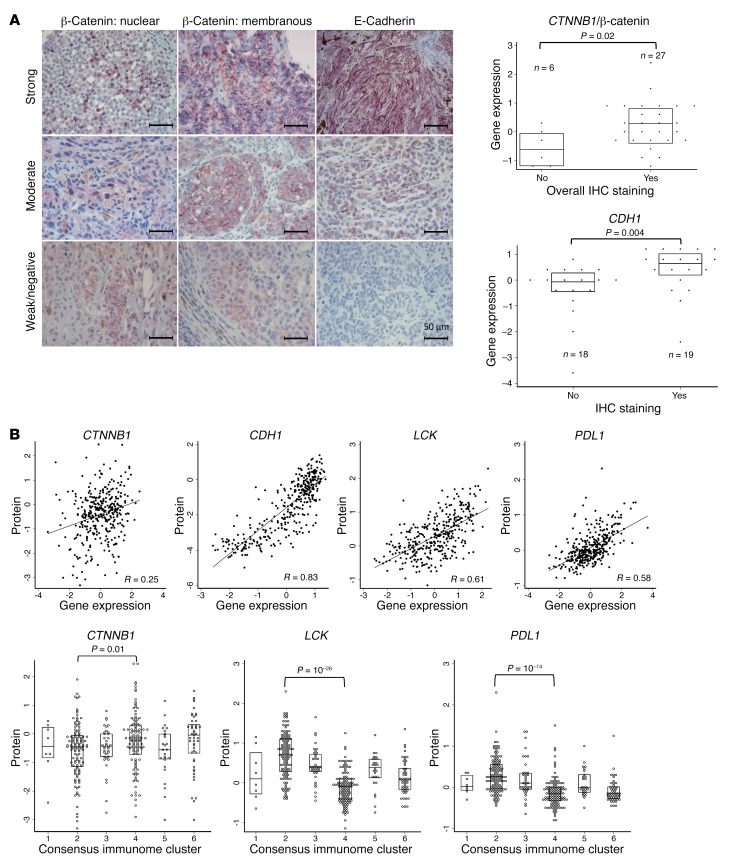
Immunotherapy prolongs survival in only a subset of melanoma patients, highlighting the need to better understand the driver tumor microenvironment. We conducted bioinformatic analyses of 703 transcriptomes to probe the immune landscape of primary cutaneous melanomas in a population-ascertained cohort. We identified and validated 6 immunologically distinct subgroups, with the largest having the lowest immune scores and the poorest survival. This poor-prognosis subgroup exhibited expression profiles consistent with β-catenin-mediated failure to recruit CD141+ DCs. A second subgroup displayed an equally bad prognosis when histopathological factors were adjusted for, while 4 others maintained comparable survival profiles. The 6 subgroups were replicated in The Cancer Genome Atlas (TCGA) melanomas, where β-catenin signaling was also associated with low immune scores predominantly related to hypomethylation. The survival benefit of high immune scores was strongest in patients with double-WT tumors for BRAF and NRAS, less strong in BRAF-V600 mutants, and absent in NRAS (codons 12, 13, 61) mutants. In summary, we report evidence for a β-catenin-mediated immune evasion in 42% of melanoma primaries overall and in 73% of those with the worst outcome. We further report evidence for an interaction between oncogenic mutations and host response to melanoma, suggesting that patient stratification will improve immunotherapeutic outcomes.
Keywords: Cancer immunotherapy; Expression profiling; Immunology; Melanoma; Oncology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
