

Accuracy and precision of ScvO2 measured with the CeVOX-device: A prospective study in patients with a wide variation of ScvO2-values
- PMID: 29664900
- PMCID: PMC5903646
- DOI: 10.1371/journal.pone.0192073
Accuracy and precision of ScvO2 measured with the CeVOX-device: A prospective study in patients with a wide variation of ScvO2-values
Abstract
Introduction: Central-venous oxygen saturation (ScvO2) is a key parameter of hemodynamic monitoring and has been suggested as therapeutic goal for resuscitation. Several devices offer continuous monitoring features. The CeVOX-device (Pulsion Medical Systems) uses a fibre-optic probe inserted through a conventional central-venous catheter (CVC) to obtain continuous ScvO2.
Objectives: Since there is a lack of studies validating the CeVOX, we prospectively analyzed data from 24 patients with CeVOX-monitoring. To increase the yield of lower ScvO2-values, 12 patients were equipped with a femoral CVC.
Methods: During the 8h study period ScvO2_CeVOX was documented immediately before withdrawal of blood to measure ScvO2 by blood gas analysis (ScvO2_BGA) 6min, 1h, 4h, 5h and 8h after the initial calibration. No further calibrations were performed.
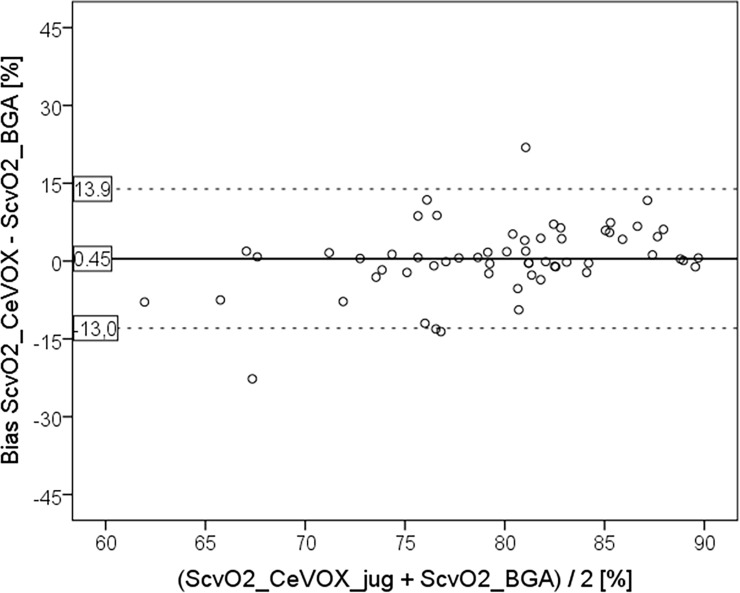
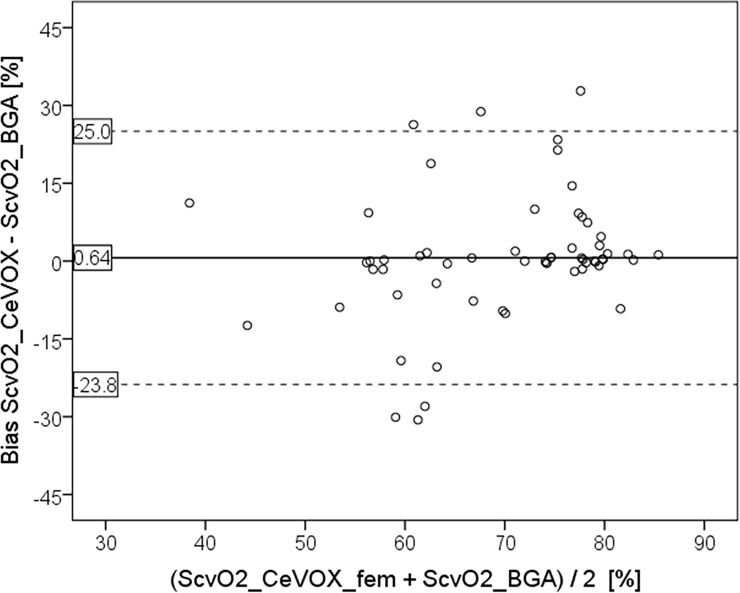
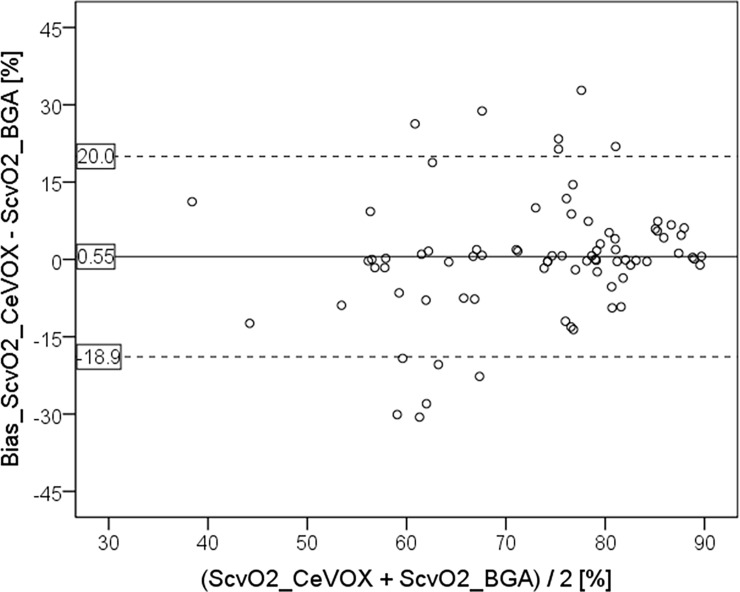
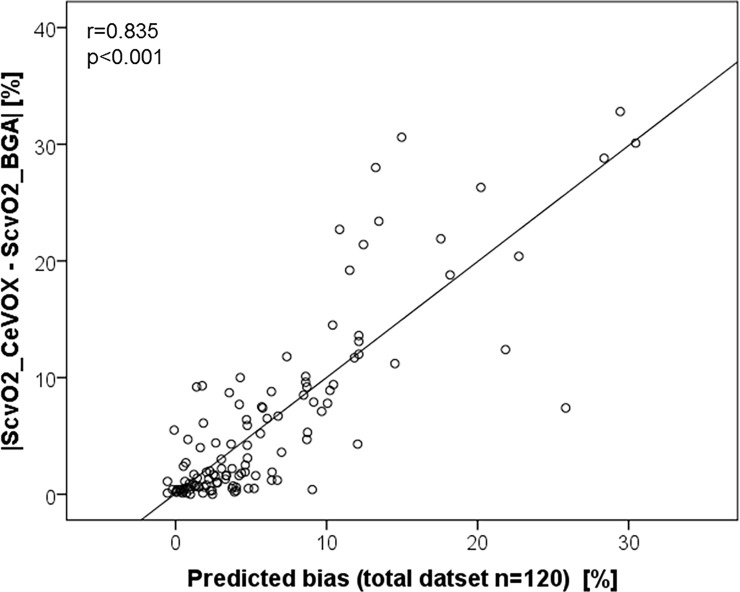
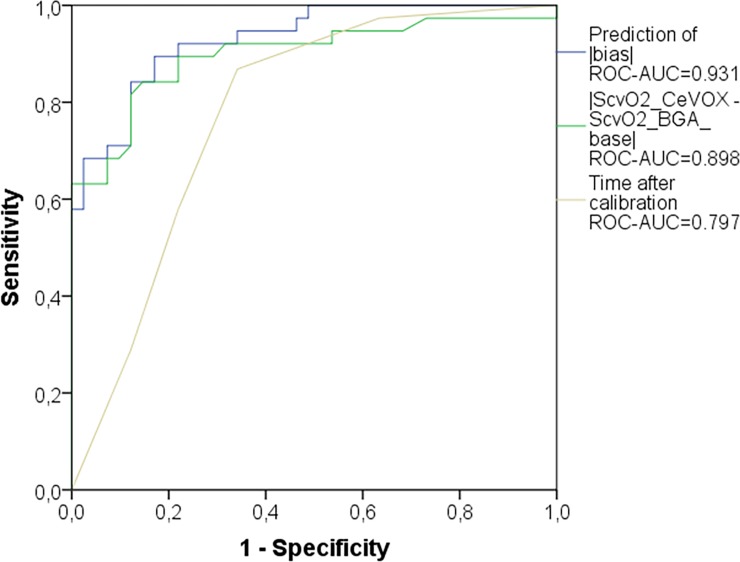
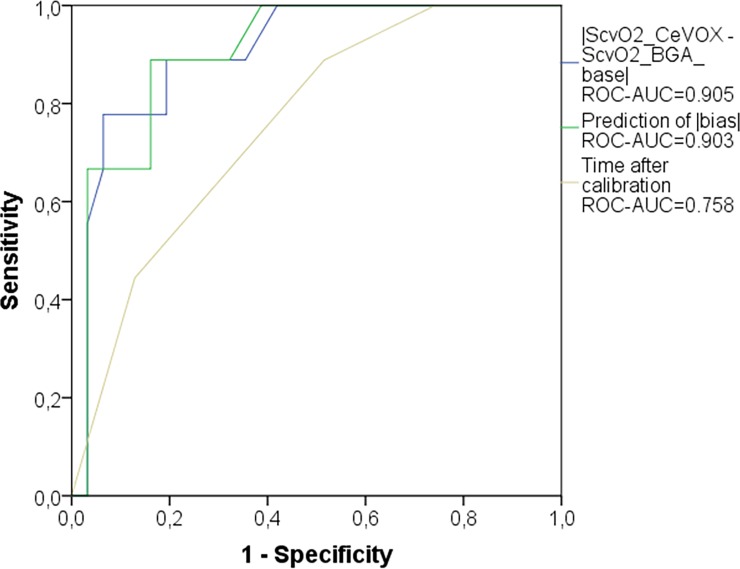
Results: In patients with jugular CVC (primary endpoint; 60 measurements), bias, lower and upper limits of agreement (LLOA; ULOA) and percentage error (PE) of the estimate of ScvO2 (ScvO2_CeVOX_jug) were acceptable with 0.45%, -13.0%, 13.9% and 16.6%, respectively. As supposed, ScvO2 was lower in the femoral compared to the jugular measurements (69.5±10.7 vs. 79.4±5.8%; p<0.001). While the bias (0.64%) was still acceptable, LLOA (-23.8%), ULOA (25.0%) and PE (34.5%) were substantially higher for femoral assessment of ScvO2 by the CeVOX (ScvO2_CeVOX_fem). Analysis of the entire data-pool with jugular as well as femoral CVCs allowed for a multivariate analysis which demonstrated that the position of the CVC per se was not independently associated with the bias ScvO2_CeVOX-ScvO2_BGA. The amount of the bias |ScvO2_CeVOX-ScvO2_BGA| was independently associated with the amount of the change of ScvO2_CeVOX compared to the initial calibration to ScvO2_BGA_baseline (|ScvO2_CeVOX-ScvO2_BGA_baseline|) as well as with low values of ScvO2_BGA_baseline. Furthermore, increasing time to the initial calibration was associated to the amount of the bias with borderline significance. A statistical model based on |ScvO2_CeVOX-ScvO2_BGA_baseline| and "time to last calibration" derived from an evaluation dataset (80 of 120 datasets, 16 of 24) provided a ROC-AUC of 0.903 to predict an amount of the bias |ScvO2_CeVOX-ScvO2_BGA| ≥5% in an independent validation group (40 datasets of 8 patients).
Conclusion: These findings suggest that the CeVOX device is capable to detect stability or instability of ScvO2_BGA. ScvO2_CeVOX accurately estimates ScvO2_BGA in case of stable values. However, intermittent measurement of ScvO2_BGA and re-calibration should be performed in case of substantial changes in ScvO2_CeVOX compared to baseline. Therefore, continuous measurement of ScvO2 with the CeVOX cannot replace ScvO2_BGA in instable patients. On the other hand, CeVOX might be useful for the monitoring of stable patients as a pre-test tool for more differentiated monitoring in case of changes in ScvO2_CeVOX.
Conflict of interest statement
Figures
Similar articles
-
Accuracy of continuous central venous oxygen saturation monitoring in patients undergoing cardiac surgery.J Clin Monit Comput. 2008 Jun;22(3):183-8. doi: 10.1007/s10877-008-9123-2. Epub 2008 Apr 29. J Clin Monit Comput. 2008. PMID: 18443743
-
Midline Catheters as an Alternative for Central Venous Catheters in Venous Oxygen Saturation Monitoring: A Single Center Experience.J Intensive Care Med. 2025 Jan;40(1):47-53. doi: 10.1177/08850666241265190. Epub 2024 Jul 23. J Intensive Care Med. 2025. PMID: 39043372
-
In vitro evaluation of the CeVOX continuous central venous oxygenation monitoring system.Anaesthesia. 2008 Apr;63(4):412-7. doi: 10.1111/j.1365-2044.2007.05376.x. Anaesthesia. 2008. PMID: 18336492
-
Utilization of Multi-Parameter Blood Gas Analysis in Prehospital Emergency Medicine-A Scoping Review.J Emerg Med. 2024 Sep;67(3):e277-e287. doi: 10.1016/j.jemermed.2024.04.014. Epub 2024 May 9. J Emerg Med. 2024. PMID: 39025715
-
Identification of data elements for blood gas analysis dataset: a base for developing registries and artificial intelligence-based systems.BMC Health Serv Res. 2022 Mar 8;22(1):317. doi: 10.1186/s12913-022-07706-y. BMC Health Serv Res. 2022. PMID: 35260155 Free PMC article. Review.
Cited by
-
Assessment of Regional Perfusion and Organ Function: Less and Non-invasive Techniques.Front Med (Lausanne). 2019 Mar 22;6:50. doi: 10.3389/fmed.2019.00050. eCollection 2019. Front Med (Lausanne). 2019. PMID: 30968023 Free PMC article. Review.
-
Do ScvO2 variations induced by passive leg raising predict fluid responsiveness? A prospective study.Physiol Rep. 2021 Sep;9(17):e15012. doi: 10.14814/phy2.15012. Physiol Rep. 2021. PMID: 34491003 Free PMC article. Clinical Trial.
-
The Various Oximetric Techniques Used for the Evaluation of Blood Oxygenation.Sensors (Basel). 2020 Aug 27;20(17):4844. doi: 10.3390/s20174844. Sensors (Basel). 2020. PMID: 32867184 Free PMC article. Review.
-
Non-invasive capnodynamic mixed venous oxygen saturation during major changes in oxygen delivery.J Clin Monit Comput. 2022 Oct;36(5):1315-1324. doi: 10.1007/s10877-021-00762-5. Epub 2021 Oct 5. J Clin Monit Comput. 2022. PMID: 34609659 Free PMC article.
-
The predictive value of lung ultrasound combined with central venous oxygen saturation variations in the outcome of ventilator weaning in patients after thoracic surgery.Am J Transl Res. 2022 Dec 15;14(12):8621-8631. eCollection 2022. Am J Transl Res. 2022. PMID: 36628206 Free PMC article.
References
-
- Rivers EP, Ander DS, Powell D (2001) Central venous oxygen saturation monitoring in the critically ill patient. Curr Opin Crit Care 7: 204–211. - PubMed
-
- Reinhart K, Kuhn HJ, Hartog C, Bredle DL (2004) Continuous central venous and pulmonary artery oxygen saturation monitoring in the critically ill. Intensive Care Med 30: 1572–1578. doi: 10.1007/s00134-004-2337-y - DOI - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, et al. (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345: 1368–1377. doi: 10.1056/NEJMoa010307 - DOI - PubMed
-
- Rady MY, Rivers EP, Nowak RM (1996) Resuscitation of the critically ill in the ED: responses of blood pressure, heart rate, shock index, central venous oxygen saturation, and lactate. Am J Emerg Med 14: 218–225. - PubMed
-
- Squara P (2014) Central venous oxygenation: when physiology explains apparent discrepancies. Crit Care 18: 579 doi: 10.1186/s13054-014-0579-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
