

Efficacy of a biomechanically-based yoga exercise program in knee osteoarthritis: A randomized controlled trial
- PMID: 29664955
- PMCID: PMC5903657
- DOI: 10.1371/journal.pone.0195653
Efficacy of a biomechanically-based yoga exercise program in knee osteoarthritis: A randomized controlled trial
Abstract
Objective: Certain exercises could overload the osteoarthritic knee. We developed an exercise program from yoga postures with a minimal knee adduction moment for knee osteoarthritis. The purpose was to compare the effectiveness of this biomechanically-based yoga exercise (YE), with traditional exercise (TE), and a no-exercise attention-equivalent control (NE) for improving pain, self-reported physical function and mobility performance in women with knee osteoarthritis.
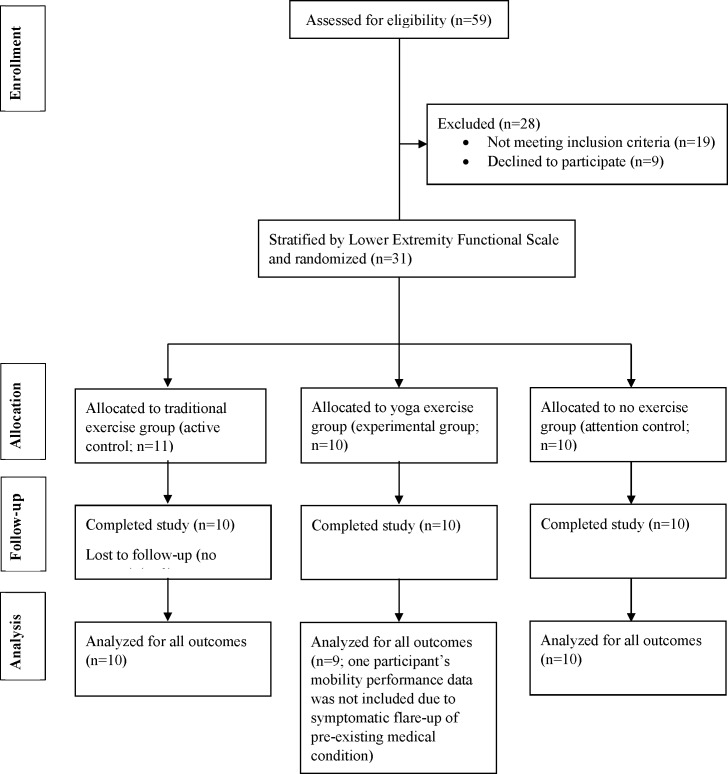
Design: Single-blind, three-arm randomized controlled trial.
Setting: Community in Southwestern Ontario, Canada.
Participants: A convenience sample of 31 women with symptomatic knee osteoarthritis was recruited through rheumatology, orthopaedic and physiotherapy clinics, newspapers and word-of-mouth.
Interventions: Participants were stratified by disease severity and randomly allocated to one of three 12-week, supervised interventions. YE included biomechanically-based yoga exercises; TE included traditional leg strengthening on machines; and NE included meditation with no exercise. Participants were asked to attend three 1-hour group classes/sessions each week.
Measurements: Primary outcomes were pain, self-reported physical function and mobility performance. Secondary outcomes were knee strength, depression, and health-related quality of life. All were assessed by a blinded assessor at baseline and immediately following the intervention.
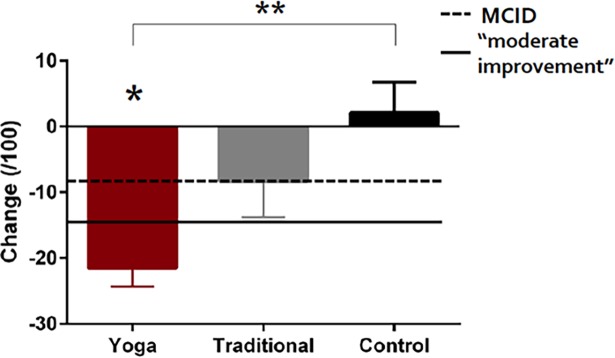
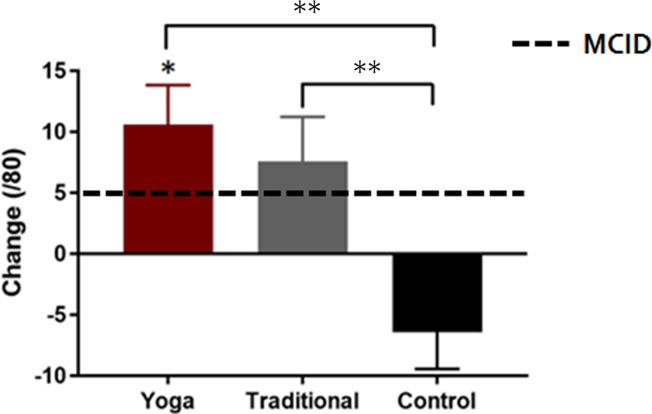
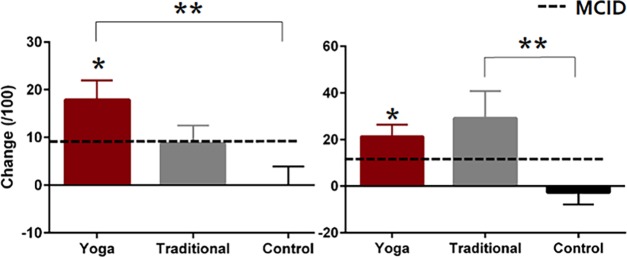
Results: The YE group demonstrated greater improvements in KOOS pain (mean difference of 22.9 [95% CI, 6.9 to 38.8; p = 0.003]), intermittent pain (mean difference of -19.6 [95% CI, -34.8 to -4.4; p = 0.009]) and self-reported physical function (mean difference of 17.2 [95% CI, 5.2 to 29.2; p = 0.003]) compared to NE. Improvements in these outcomes were similar between YE and TE. However, TE demonstrated a greater improvement in knee flexor strength compared to YE (mean difference of 0.1 [95% CI, 0.1 to 0.2]. Improvements from baseline to follow-up were present in quality of life score for YE and knee flexor strength for TE, while both also demonstrated improvements in mobility. No improvement in any outcome was present in NE.
Conclusions: The biomechanically-based yoga exercise program produced clinically meaningful improvements in pain, self-reported physical function and mobility in women with clinical knee OA compared to no exercise. While not statistically significant, improvements in these outcomes were larger than those elicited from the traditional exercise-based program. Though this may suggest that the yoga program may be more efficacious for knee OA, future research studying a larger sample is required.
Trial registration: ClinicalTrials.gov (NCT02370667).
Conflict of interest statement
Figures
References
-
- Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64 doi: 10.1186/1477-7525-1-64 - DOI - PMC - PubMed
-
- Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee In: The Cochrane Collaboration, editor. Cochrane Database of Systematic Reviews [Internet]. Chichester, UK: John Wiley & Sons, Ltd; 2015. [cited 2015 Jan 27]. Available from: http://doi.wiley.com/10.1002/14651858.CD004376.pub3 - DOI
-
- Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012. April;64(4):465–74. - PubMed
-
- Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008. February;16(2):137–62. doi: 10.1016/j.joca.2007.12.013 - DOI - PubMed
-
- Bennell KL, Bowles K-A, Wang Y, Cicuttini F, Davies-Tuck M, Hinman RS. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Ann Rheum Dis. 2011. October;70(10):1770–4. doi: 10.1136/ard.2010.147082 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
