

Contemporary survival of patients with pulmonary arterial hypertension and congenital systemic to pulmonary shunts
- PMID: 29664959
- PMCID: PMC5903600
- DOI: 10.1371/journal.pone.0195092
Contemporary survival of patients with pulmonary arterial hypertension and congenital systemic to pulmonary shunts
Abstract
Objective: To compare survival of patients with newly diagnosed pulmonary arterial hypertension associated with congenital heart disease (PAH-CHD) according to various clinical classifications with classifications of anatomical-pathophysiological systemic to pulmonary shunts in a single-center cohort.
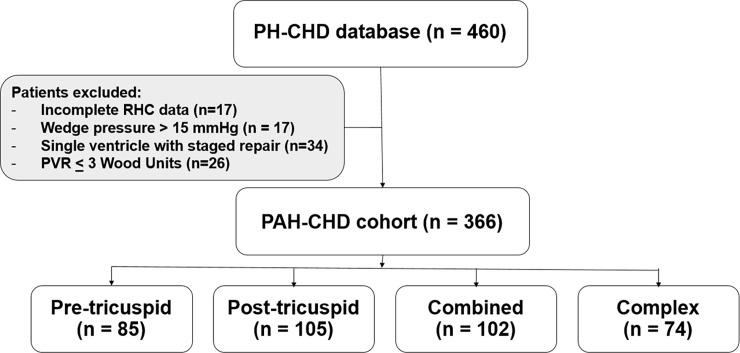
Methods: All prevalent cases of PAH-CHD with hemodynamic confirmation by cardiac catheterization in 1995-2015 were retrospectively reviewed. Patients who were younger than three months of age, or with single ventricle following surgery were excluded. Baseline characteristics and clinical outcomes were retrieved from the database. The survival analysis was performed at the end of 2016. Prognostic factors were identified using multivariate analysis.
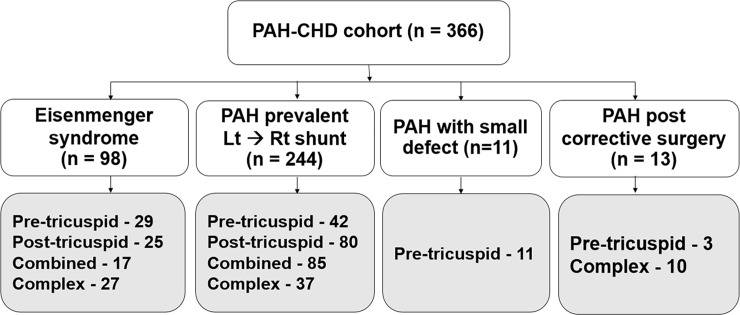
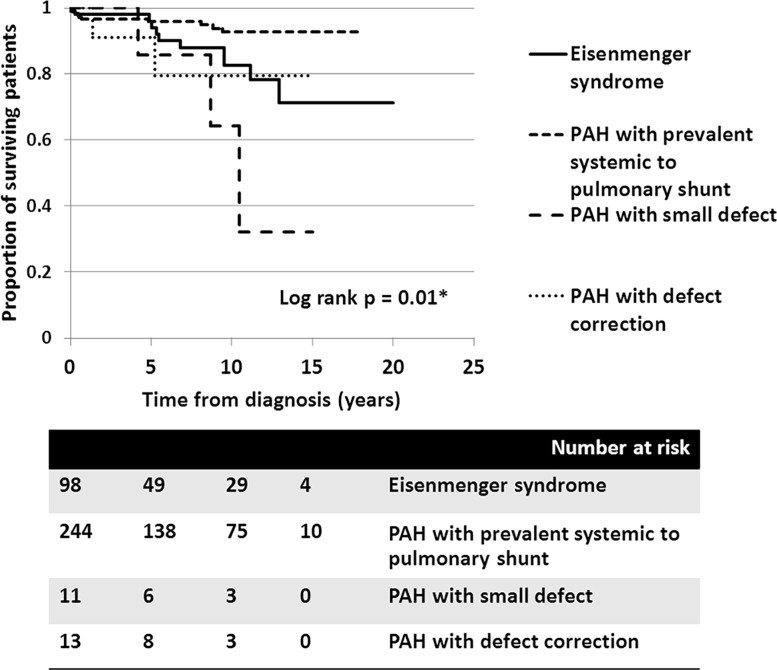
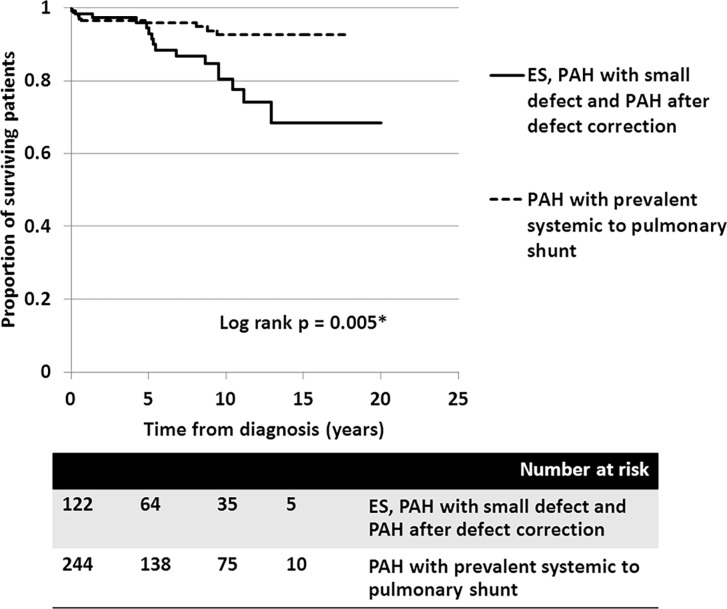
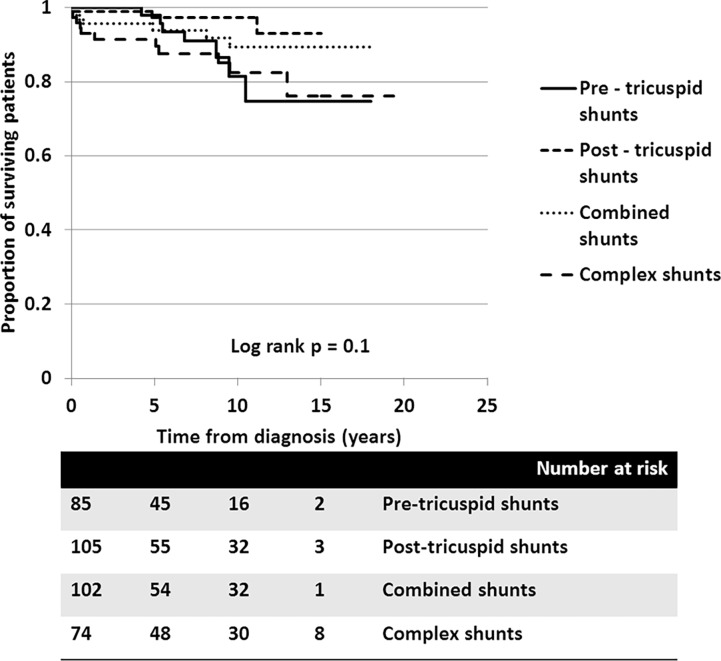
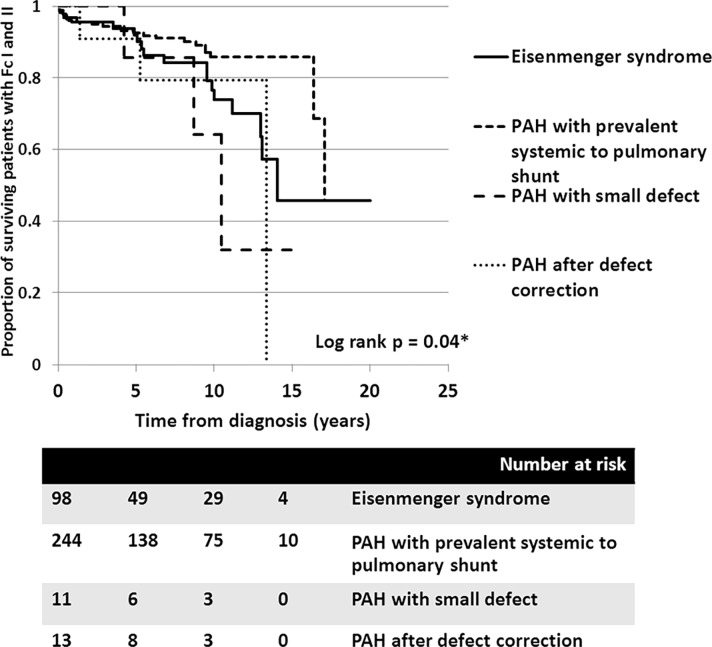
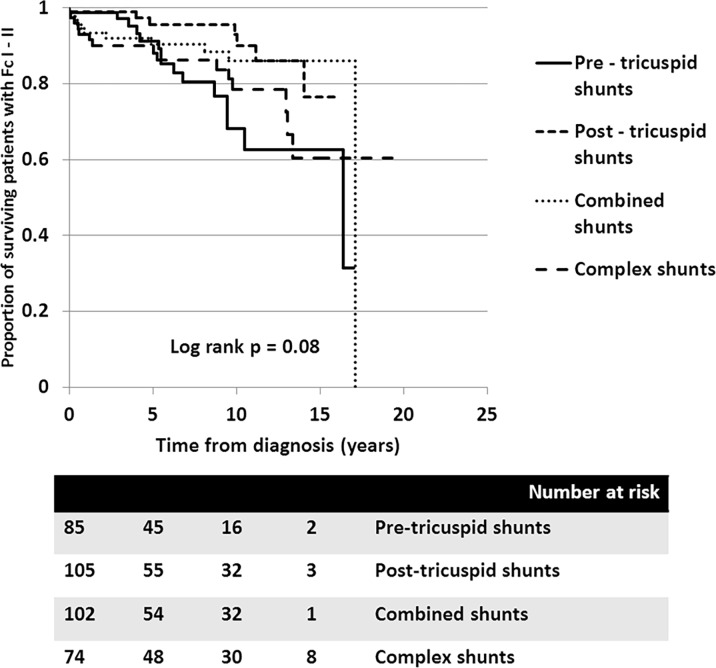
Results: A total of 366 consecutive patients (24.5 ± 17.6 years of age, 40% male) with PAH-CHD were analyzed. Most had simple shunts (85 pre-tricuspid, 105 post-tricuspid, 102 combined shunts). Patients with pre-tricuspid shunts were significantly older at diagnosis in comparison to post-tricuspid, combined, and complex shunts. Clinical classifications identified patients as having Eisenmenger syndrome (ES, 26.8%), prevalent left to right shunt (66.7%), PAH with small defect (3%), or PAH following defect correction (3.5%). At follow-up (median = 5.9 years; 0.1-20.7 years), no statistically significant differences in survival rate were seen among the anatomical-pathophysiological shunts (p = 0.1). Conversely, the clinical classifications revealed that patients with PAH-small defect had inferior survival compared to patients with ES, PAH post-corrective surgery, or PAH with prevalent left to right shunt (p = 0.01). Significant mortality risks were functional class III, age < 10 years, PAH-small defect, elevated right atrial pressure > 15 mmHg, and baseline PVR > 8 WU•m.2.
Conclusion: Patients with PAH-CHD had a modest long-term survival. Different anatomical-pathophysiological shunts affect the natural presentation, while clinical classifications indicate treatment strategies and survival. Contemporary therapy improves survival in deliberately selected patients.
Conflict of interest statement
Figures
References
-
- Galie N, Torbicki A, Barst R, Dartevelle P, Haworth S, Higenbottam T, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension. The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J. 2004;25(24):2243–78. Epub 2004/12/14. doi: 10.1016/j.ehj.2004.09.014 . - DOI - PubMed
-
- Hoeper MM, Bogaard HJ, Condliffe R, Frantz R, Khanna D, Kurzyna M, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D42–50. Epub 2013/12/21. doi: 10.1016/j.jacc.2013.10.032 . - DOI - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D34–41. Epub 2013/12/21. doi: 10.1016/j.jacc.2013.10.029 . - DOI - PubMed
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. Epub 2015/09/01. doi: 10.1093/eurheartj/ehv317 . - DOI - PubMed
-
- Duffels MG, Engelfriet PM, Berger RM, van Loon RL, Hoendermis E, Vriend JW, et al. Pulmonary arterial hypertension in congenital heart disease: an epidemiologic perspective from a Dutch registry. Int J Cardiol. 2007;120(2):198–204. Epub 2006/12/22. doi: 10.1016/j.ijcard.2006.09.017 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
