

Deep learning improves prediction of drug-drug and drug-food interactions
- PMID: 29666228
- PMCID: PMC5939113
- DOI: 10.1073/pnas.1803294115
Deep learning improves prediction of drug-drug and drug-food interactions
Abstract
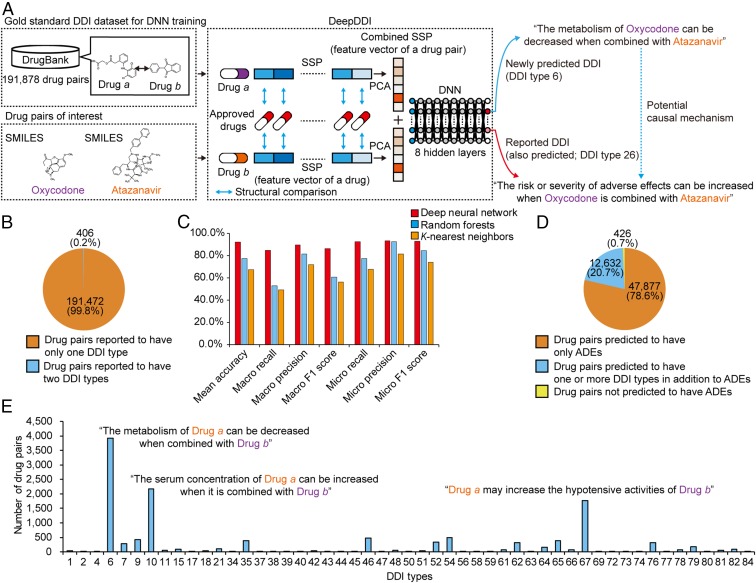
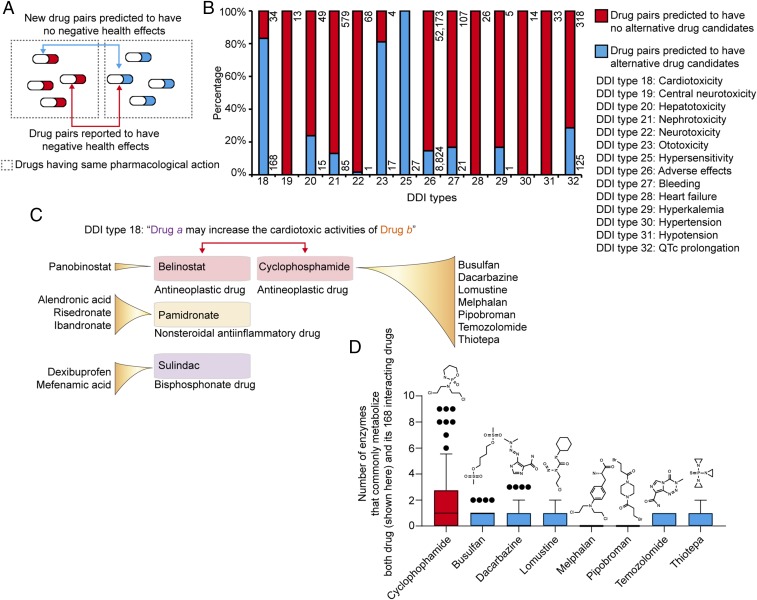
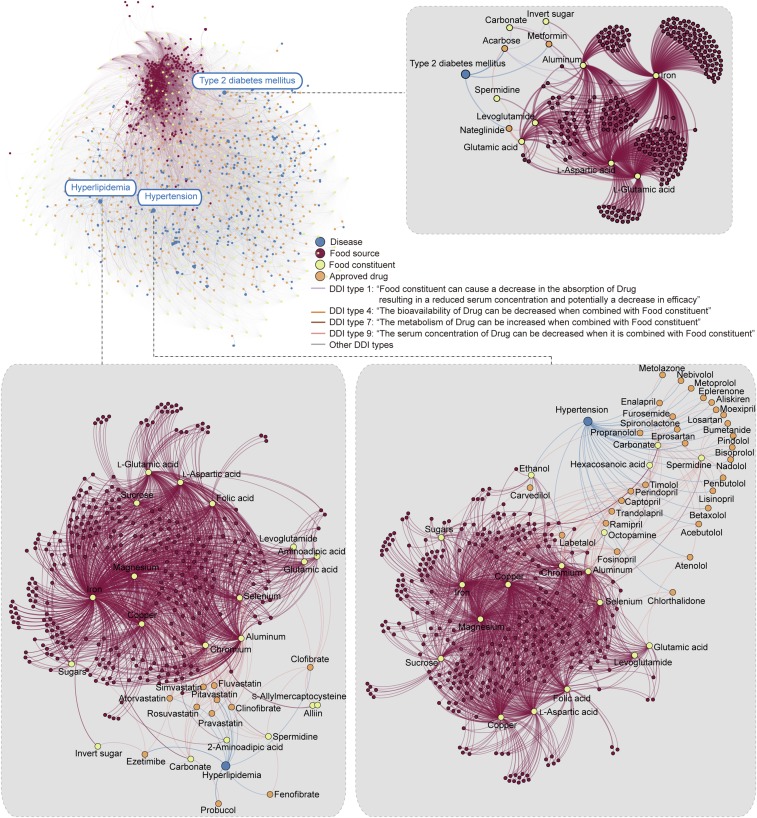
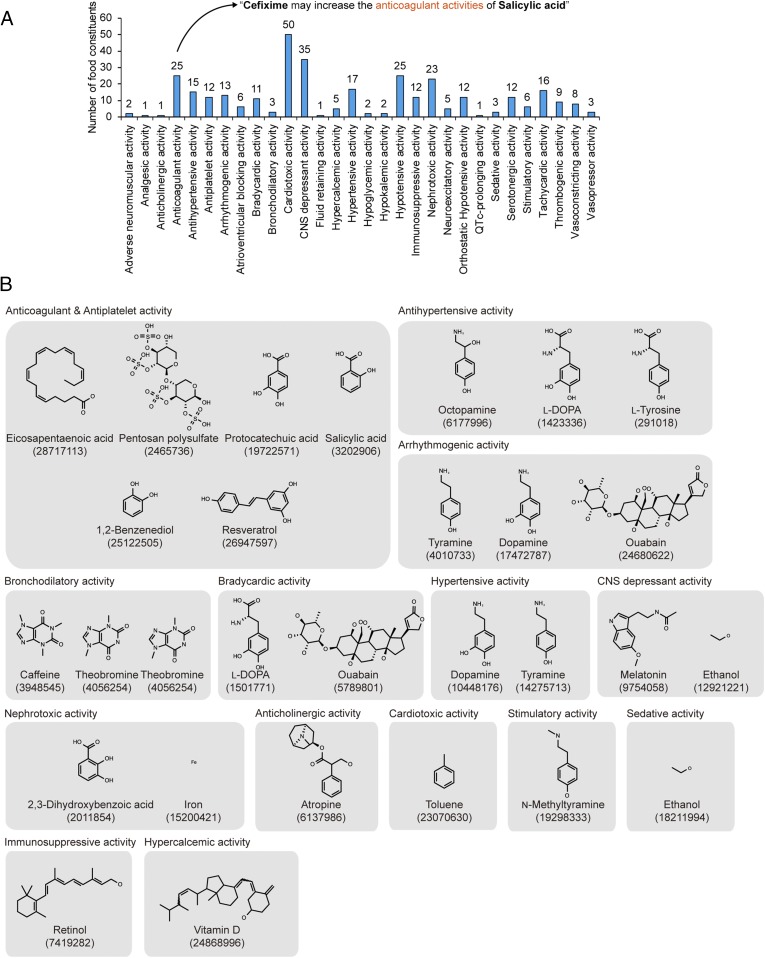
Drug interactions, including drug-drug interactions (DDIs) and drug-food constituent interactions (DFIs), can trigger unexpected pharmacological effects, including adverse drug events (ADEs), with causal mechanisms often unknown. Several computational methods have been developed to better understand drug interactions, especially for DDIs. However, these methods do not provide sufficient details beyond the chance of DDI occurrence, or require detailed drug information often unavailable for DDI prediction. Here, we report development of a computational framework DeepDDI that uses names of drug-drug or drug-food constituent pairs and their structural information as inputs to accurately generate 86 important DDI types as outputs of human-readable sentences. DeepDDI uses deep neural network with its optimized prediction performance and predicts 86 DDI types with a mean accuracy of 92.4% using the DrugBank gold standard DDI dataset covering 192,284 DDIs contributed by 191,878 drug pairs. DeepDDI is used to suggest potential causal mechanisms for the reported ADEs of 9,284 drug pairs, and also predict alternative drug candidates for 62,707 drug pairs having negative health effects. Furthermore, DeepDDI is applied to 3,288,157 drug-food constituent pairs (2,159 approved drugs and 1,523 well-characterized food constituents) to predict DFIs. The effects of 256 food constituents on pharmacological effects of interacting drugs and bioactivities of 149 food constituents are predicted. These results suggest that DeepDDI can provide important information on drug prescription and even dietary suggestions while taking certain drugs and also guidelines during drug development.
Keywords: DeepDDI; deep learning; drug–drug interactions; drug–food interactions; structural similarity profile.
Conflict of interest statement
Conflict of interest statement: The authors and sponsor declare the technology described here is patent filed (KR-10-2017-0164115) for potential commercialization.
Figures
References
-
- Edwards IR, Aronson JK. Adverse drug reactions: Definitions, diagnosis, and management. Lancet. 2000;356:1255–1259. - PubMed
-
- Pirmohamed M, Orme M. Drug Interactions of Clinical Importance. Chapman & Hall; London: 1998. pp. 888–912.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
