

Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis
- PMID: 29666906
- PMCID: PMC6021475
- DOI: 10.1007/s00270-018-1959-3
Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis
Abstract
Purpose: To assess safety and outcome of radiofrequency ablation (RFA) and microwave ablation (MWA) as compared to systemic chemotherapy and partial hepatectomy (PH) in the treatment of colorectal liver metastases (CRLM).
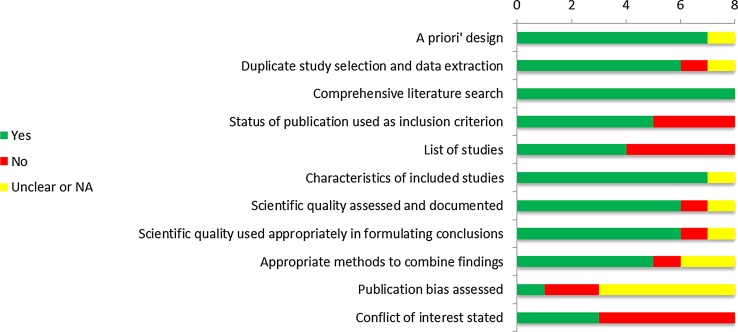
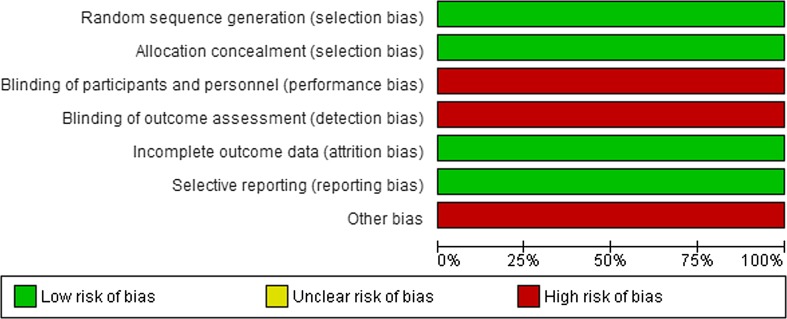
Methods: MEDLINE, Embase and the Cochrane Library were searched. Randomized trials and comparative observational studies with multivariate analysis and/or matching were included. Guidelines from National Guideline Clearinghouse and Guidelines International Network were assessed using the AGREE II instrument.
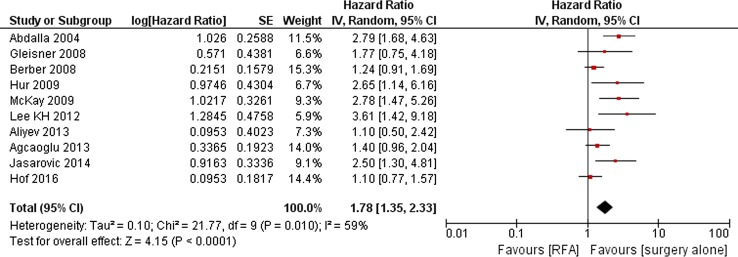
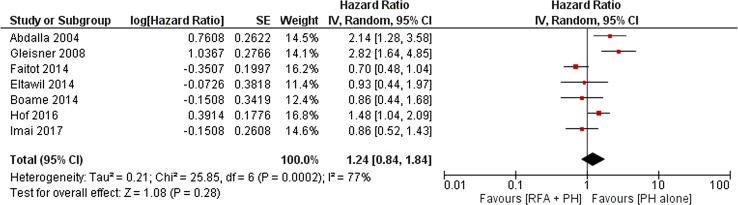
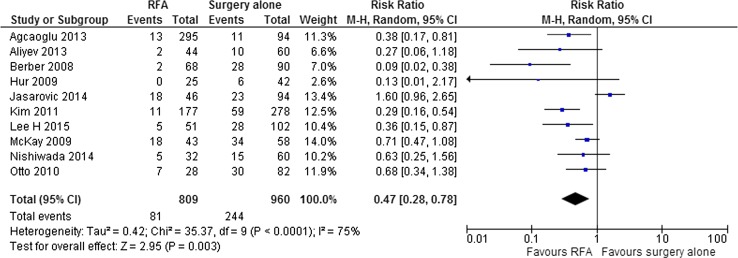
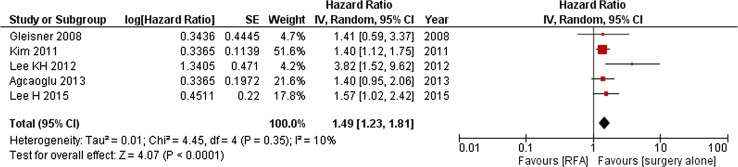
Results: The search revealed 3530 records; 328 were selected for full-text review; 48 were included: 8 systematic reviews, 2 randomized studies, 26 comparative observational studies, 2 guideline-articles and 10 case series; in addition 13 guidelines were evaluated. Literature to assess the effectiveness of ablation was limited. RFA + systemic chemotherapy was superior to chemotherapy alone. PH was superior to RFA alone but not to RFA + PH or to MWA. Compared to PH, RFA showed fewer complications, MWA did not. Outcomes were subject to residual confounding since ablation was only employed for unresectable disease.
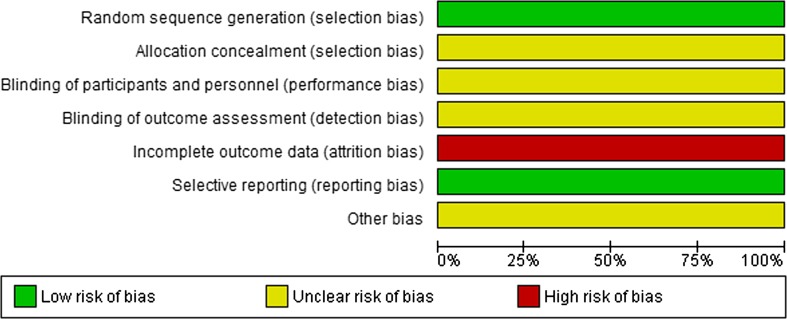
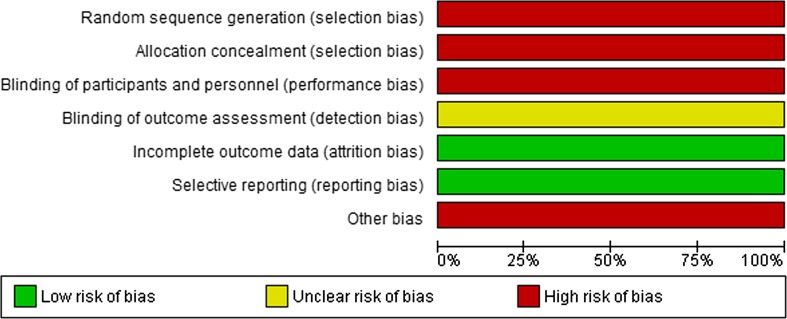
Conclusion: The results from the EORTC-CLOCC trial, the comparable survival for ablation + PH versus PH alone, the potential to induce long-term disease control and the low complication rate argue in favour of ablation over chemotherapy alone. Further randomized comparisons of ablation to current-day chemotherapy alone should therefore be considered unethical. Hence, the highest achievable level of evidence for unresectable CRLM seems reached. The apparent selection bias from previous studies and the superior safety profile mandate the setup of randomized controlled trials comparing ablation to surgery.
Keywords: Colorectal liver metastases (CRLM); Microwave ablation (MWA); Partial hepatectomy (PH); Radiofrequency ablation (RFA); Systemic chemotherapy.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures








References
-
- Bala MM, Riemsma RP, Wolff R, Kleijnen J. Microwave coagulation for liver metastases. Cochrane Database Syst Rev. 2013;(10):CD010163. - PubMed
-
- Belinson S, Chopra R, Yang Y, Shankaran V, Aronson N. Local hepatic therapies for metastases to the liver from unresectable colorectal cancer. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012:13-EHC014-EF. - PubMed
-
- Maindrault-Goebel F, de Gramont A, Louvet C, et al. Evaluation of oxaliplatin dose intensity in bimonthly leucovorin and 48-hour 5-fluorouracil continuous infusion regimens (FOLFOX) in pretreated metastatic colorectal cancer. Oncology Multidisciplinary Research Group (GERCOR) Ann Oncol. 2000;11(11):1477–1483. doi: 10.1023/A:1026520812351. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
