

Treatment in a preventive cardiology clinic utilizing advanced practice providers effectively closes atherosclerotic cardiovascular disease risk-management gaps among a primary-prevention population compared with a propensity-matched primary-care cohort: A team-based care model and its impact on lipid and blood pressure management
- PMID: 29667200
- PMCID: PMC6489740
- DOI: 10.1002/clc.22963
Treatment in a preventive cardiology clinic utilizing advanced practice providers effectively closes atherosclerotic cardiovascular disease risk-management gaps among a primary-prevention population compared with a propensity-matched primary-care cohort: A team-based care model and its impact on lipid and blood pressure management
Abstract
Background: Advanced practice providers (APPs) can fill care gaps created by physician shortages and improve adherence/compliance with preventive ASCVD interventions.
Hypothesis: APPs utilizing guideline-based algorithms will more frequently escalate ASCVD risk factor therapies.
Methods: We retrospectively reviewed data on 595 patients enrolled in a preventive cardiology clinic (PCC) utilizing APPs compared with a propensity-matched cohort (PMC) of 595 patients enrolled in primary-care clinics alone. PCC patients were risk-stratified using Framingham Risk Score (FRS) and coronary artery calcium scoring (CACS).
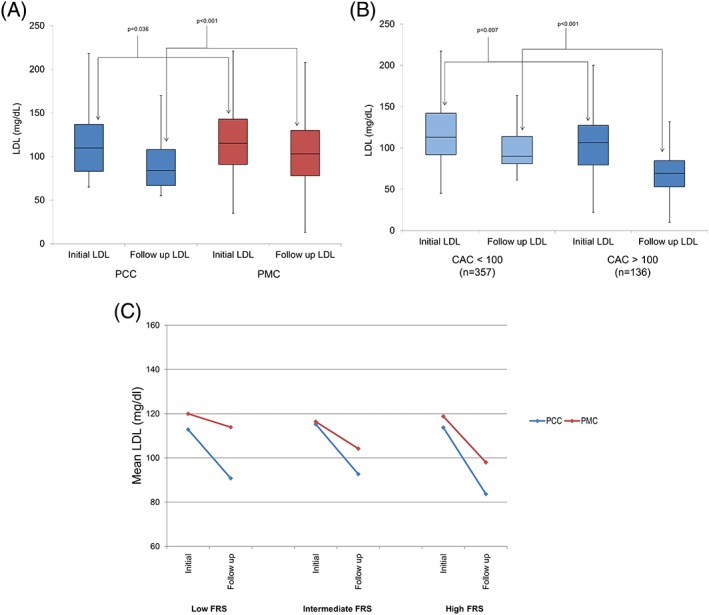
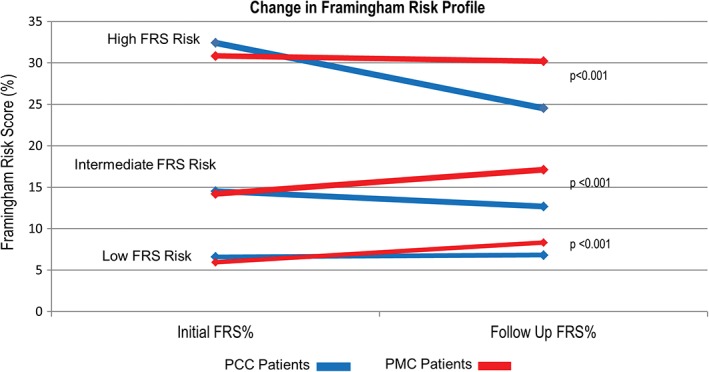
Results: Baseline demographics were balanced between the groups. CACS was more commonly obtained in PCC patients (P < 0.001), resulting in reclassification of 30.6% patients to a higher risk category, including statin therapy in 26.6% of low-FRS PCC patients with CACS ≥75th MESA percentile. Aspirin initiation was higher for high and intermediate FRS patients in the PCC (P < 0.001). Post-intervention mean LDL-C, non-HDL-C, and triglycerides (all P < 0.05) were lower in the PCC group. Compliance with appropriate lipid treatment was higher in intermediate to high FRS patients (P = 0.004) in the PCC group. Aggressive LDL-C and non-HDL-C treatment goals (<70 mg/dL, P = 0.005 and < 130 mg/dL, P < 0.001, respectively), were more commonly achieved in high-FRS PCC patients. Median post-intervention SBP was lower among intermediate and low FRS patients (P = 0.001 and P < 0.001, respectively). Cumulatively, this resulted in a reduction in median post-intervention PCC FRS across all initial FRS risk categories (P < 0.001 for all).
Conclusions: APPs within a PCC effectively risk-stratify and aggressively manage ASCVD risk factors, resulting in a reduction in post-intervention FRS.
Keywords: Atherosclerosis; Blood Pressure Control and Regulation; Computed Tomography; General Clinical Cardiology/Adult; Imaging; Preventive Cardiology.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The views expressed herein are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, the Department of Defense or the U.S. government. The authors declare no potential conflicts of interest.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Executive summary: Heart Disease and Stroke Statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133:447–454. - PubMed
-
- Domanski M, Lloyd‐Jones D, Fuster V, et al. Can we dramatically reduce the incidence of coronary heart disease? Nat Rev Cardiol. 2011;8:721–725. - PubMed
-
- Maddox TM, Borden WB, Tang F, et al. Implications of the 2013 ACC/AHA cholesterol guidelines for adults in contemporary cardiovascular practice: insights from the NCDR PINNACLE registry. J Am Coll Cardiol. 2014;64:2183–2192. - PubMed
-
- Rodgers GP, Conti JB, Feinstein JA, et al. ACC 2009 survey results and recommendations: addressing the cardiology workforce crisis: a report of the ACC Board of Trustees Workforce Task Force. J Am Coll Cardiol. 2009;54:1195–1208. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
