

Alectinib versus chemotherapy in crizotinib-pretreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer: results from the phase III ALUR study
- PMID: 29668860
- PMCID: PMC6005013
- DOI: 10.1093/annonc/mdy121
Alectinib versus chemotherapy in crizotinib-pretreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer: results from the phase III ALUR study
Abstract
Background: This is the first trial to directly compare efficacy and safety of alectinib versus standard chemotherapy in advanced/metastatic anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer (NSCLC) patients who have progressed on, or were intolerant to, crizotinib.
Patients and methods: ALUR (MO29750; NCT02604342) was a randomized, multicenter, open-label, phase III trial of alectinib versus chemotherapy in advanced/metastatic ALK-positive NSCLC patients previously treated with platinum-based doublet chemotherapy and crizotinib. Patients were randomized 2 : 1 to receive alectinib 600 mg twice daily or chemotherapy (pemetrexed 500 mg/m2 or docetaxel 75 mg/m2, both every 3 weeks) until disease progression, death, or withdrawal. Primary end point was investigator-assessed progression-free survival (PFS).
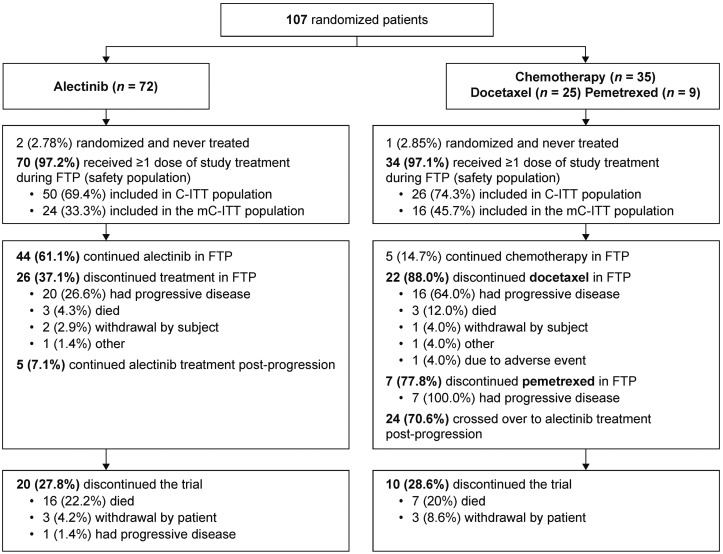
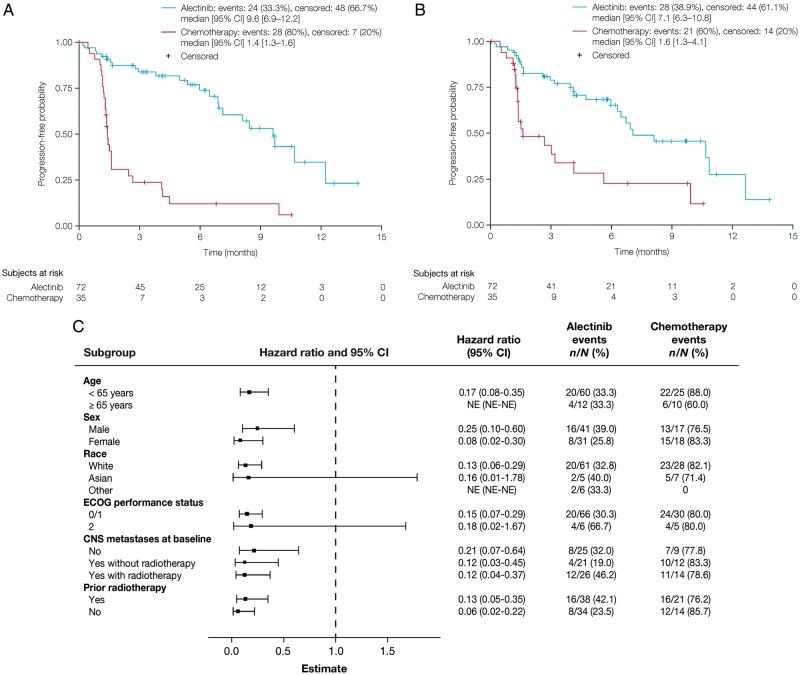
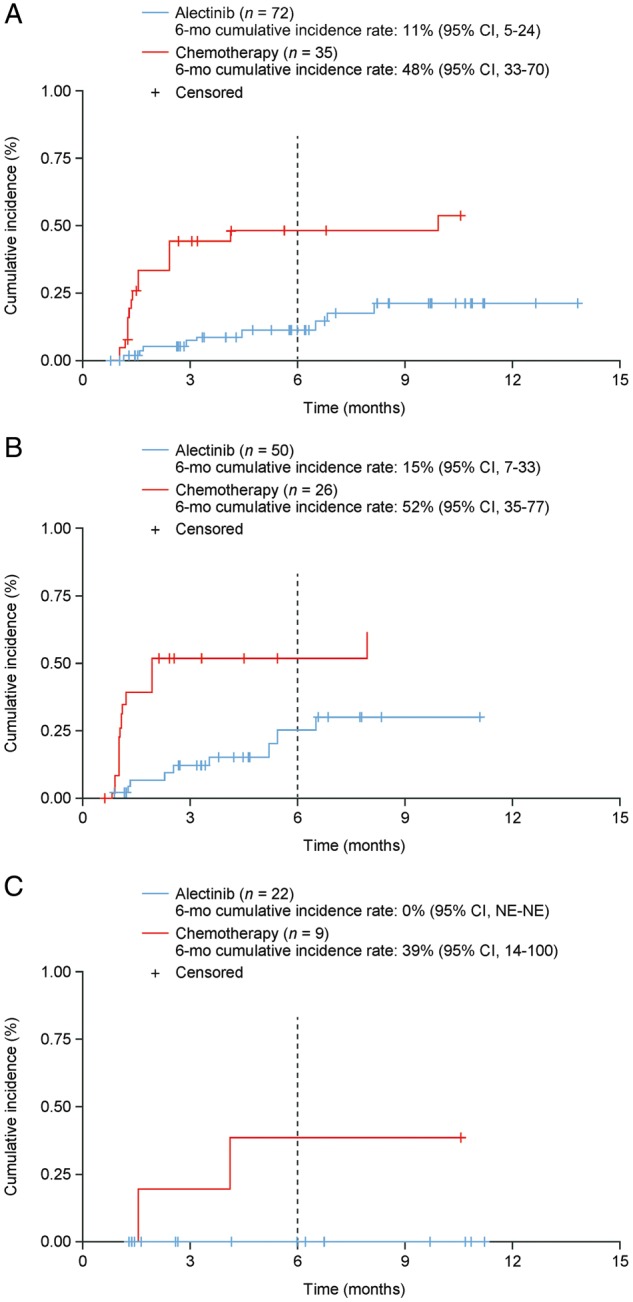
Results: Altogether, 107 patients were randomized (alectinib, n = 72; chemotherapy, n = 35) in 13 countries across Europe and Asia. Median investigator-assessed PFS was 9.6 months [95% confidence interval (CI): 6.9-12.2] with alectinib and 1.4 months (95% CI: 1.3-1.6) with chemotherapy [hazard ratio (HR) 0.15 (95% CI: 0.08-0.29); P < 0.001]. Independent Review Committee-assessed PFS was also significantly longer with alectinib [HR 0.32 (95% CI: 0.17-0.59); median PFS was 7.1 months (95% CI: 6.3-10.8) with alectinib and 1.6 months (95% CI: 1.3-4.1) with chemotherapy]. In patients with measurable baseline central nervous system (CNS) disease (alectinib, n = 24; chemotherapy, n = 16), CNS objective response rate was significantly higher with alectinib (54.2%) versus chemotherapy (0%; P < 0.001). Grade ≥3 adverse events were more common with chemotherapy (41.2%) than alectinib (27.1%). Incidence of AEs leading to study-drug discontinuation was lower with alectinib (5.7%) than chemotherapy (8.8%), despite alectinib treatment duration being longer (20.1 weeks versus 6.0 weeks).
Conclusion: Alectinib significantly improved systemic and CNS efficacy versus chemotherapy for crizotinib-pretreated ALK-positive NSCLC patients, with a favorable safety profile.
Trial registration: ClinicalTrials.gov NCT02604342; Roche study MO29750.
Figures
Comment in
-
The allure of 'ALUR'.Ann Oncol. 2018 Jun 1;29(6):1344-1346. doi: 10.1093/annonc/mdy144. Ann Oncol. 2018. PMID: 29688274 No abstract available.
References
-
- FDA Approval for Ceritinib. https://www.cancer.gov/about-cancer/treatment/drugs/fda-ceritinib (March 2018, date last accessed).
-
- EMA Zykadia recommended for approval in advanced nonsmall-cell lung cancer. http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2... (March 2018, date last accessed).
-
- Stenger M. Ceritinib in ALK-positive metastatic NSCLC patients with progression on or intolerance to crizotinib. The ASCO Post 10 June 2014, Volume 5, Issue 9. http://www.ascopost.com/issues/june-10,-2014/ceritinib-in-alkpositive-me... (March 2018, date last accessed).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
