

Predictors of Durability of Radiological Response in Patients With Small Bowel Crohn's Disease
- PMID: 29668921
- PMCID: PMC6391864
- DOI: 10.1093/ibd/izy074
Predictors of Durability of Radiological Response in Patients With Small Bowel Crohn's Disease
Abstract
Background: The long-term significance of radiological transmural response (TR) as a treatment goal at the first follow-up scan in small bowel Crohn's disease (CD) has been previously shown. We examined the durability of a long-term strategy of treating to a target of radiological TR and the influence of baseline predictors on the maintenance of TR.
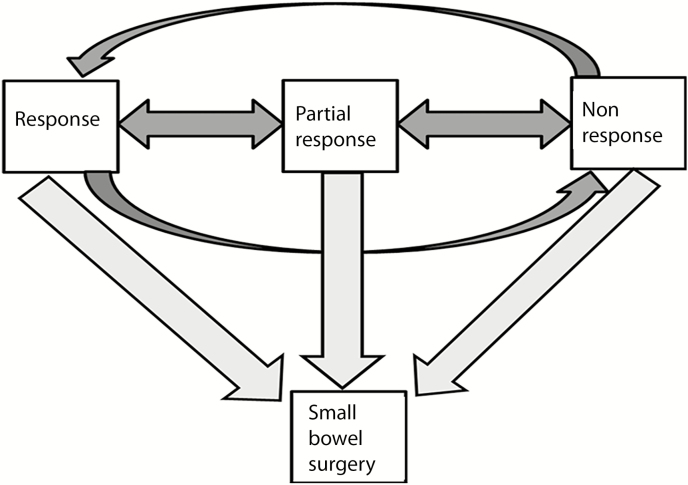
Methods: Small bowel CD patients between January 1, 2002, and December 31, 2014, were identified with serial computed tomography enterography (CTE)/magnetic resonance enterography (MRE) before and after initiation of therapy or on maintenance therapy. Overall TR (inflammatory lesions with/without strictures) w1as characterized by abdominal radiologists in up to 5 small bowel lesions per patient at each serial scan until last follow-up or small bowel resection, as response, partial response, or nonresponse. The rate of conversion between TR states and transition to surgery, including the effect of baseline patient/disease characteristics, was examined using a multistate model (mstate R-package).
Results: CD patients (n = 150, 705 CTE/MRE) with a median of 4 CTE/MRE during 4.6 years of follow-up, 49% with ileal-only distribution, had 260 examined bowel segments. Conversion from response to partial response/nonresponse was 37.4% per year of follow-up with no transitions seen directly from response to surgery. Current smoking status (hazard ratio [HR], 2.2; 95% confidence interval [CI], 1.1-4.3) and internal penetrating disease at baseline scan (HR, 2.2; 95% CI, 1.2-4.1) were associated with a 2-fold increased risk of transition from partial response/nonresponse to surgery.
Conclusions: Achievement and maintenance of radiological response is associated with avoidance of small bowel surgery. Continued follow-up with CTE/MRE is recommended to identify loss of response, especially in current smokers and patients with internal penetrating disease at baseline CTE/MRE.
Figures
References
-
- Podolsky DK. Inflammatory bowel disease (1). N Engl J Med. 1991;325:928–37. - PubMed
-
- Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, et al. . The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–97. - PubMed
-
- Peyrin-Biroulet L, Reinisch W, Colombel JF, et al. . Clinical disease activity, C-reactive protein normalisation and mucosal healing in Crohn’s disease in the SONIC trial. Gut. 2014;63:88–95. - PubMed
-
- Cellier C, Sahmoud T, Froguel E, et al. . Correlations between clinical activity, endoscopic severity, and biological parameters in colonic or ileocolonic Crohn’s disease. a prospective multicentre study of 121 cases. The Groupe d’Etudes Thérapeutiques des Affections Inflammatoires Digestives. Gut. 1994;35:231–5. - PMC - PubMed
-
- Siddiki HA, Fidler JL, Fletcher JG, et al. . Prospective comparison of state-of-the-art MR enterography and CT enterography in small-bowel Crohn’s disease. Am J Roentgenol. 2009;193:113–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
