

Current Challenges and Opportunities in Treating Glioblastoma
- PMID: 29669750
- PMCID: PMC5907910
- DOI: 10.1124/pr.117.014944
Current Challenges and Opportunities in Treating Glioblastoma
Abstract
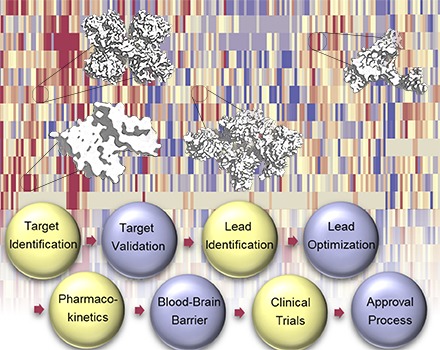
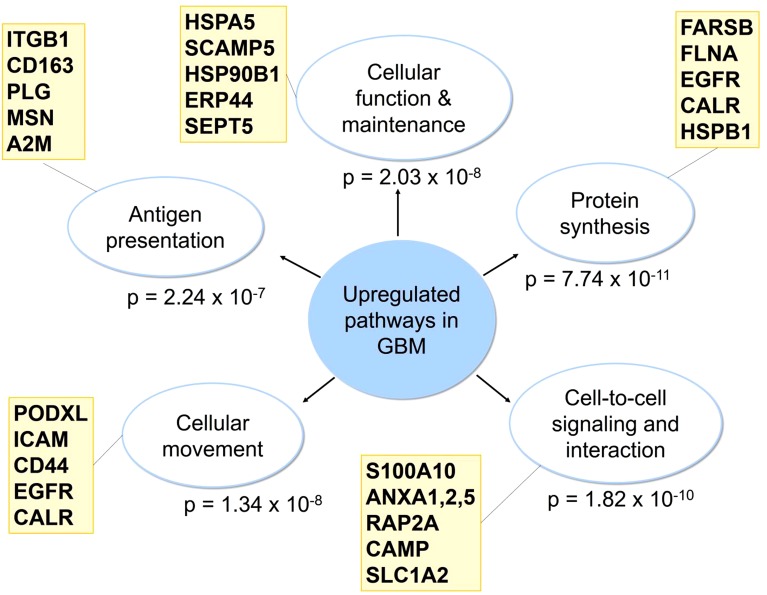
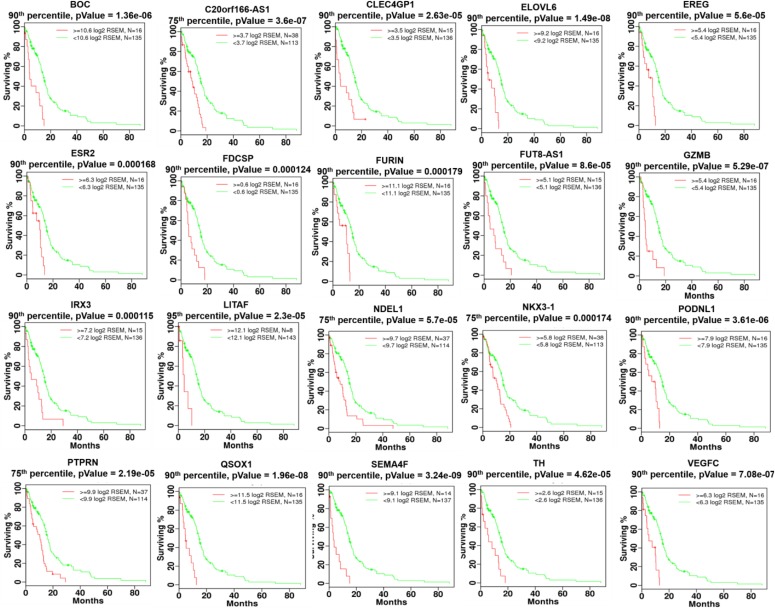
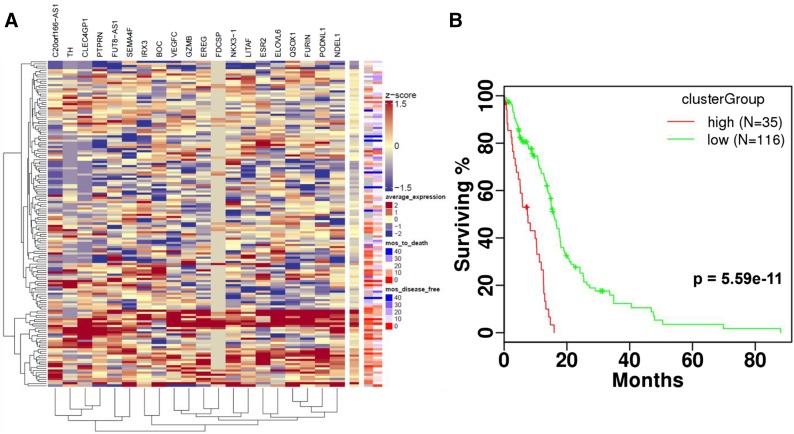
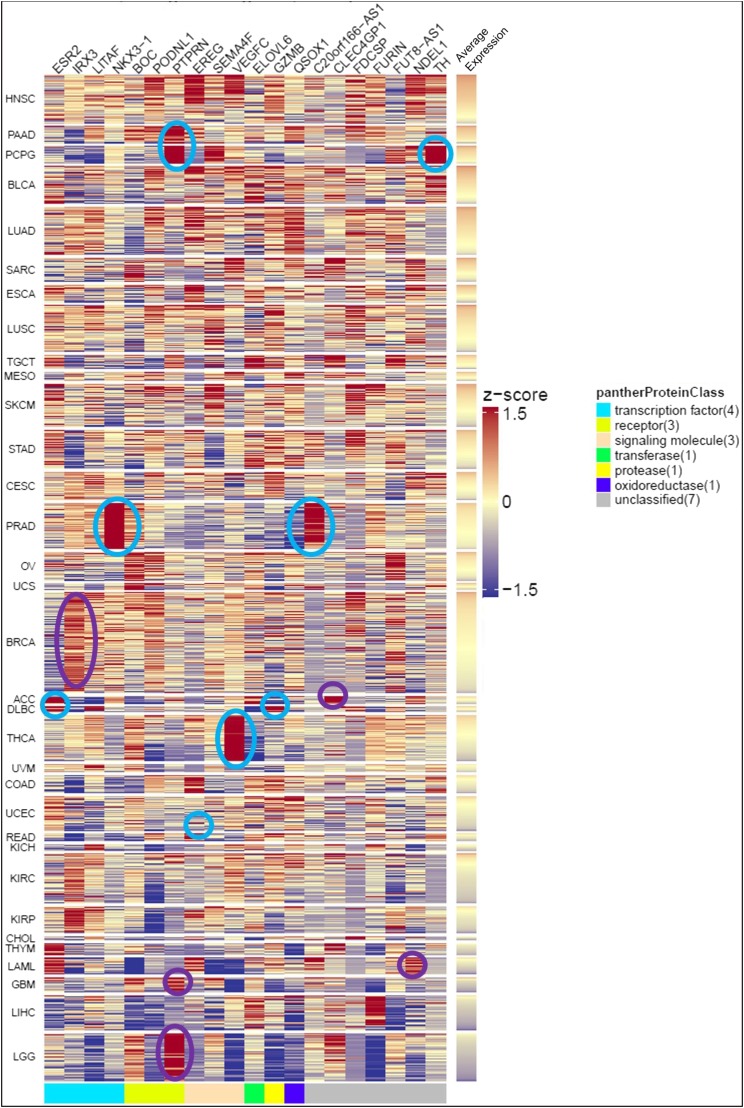
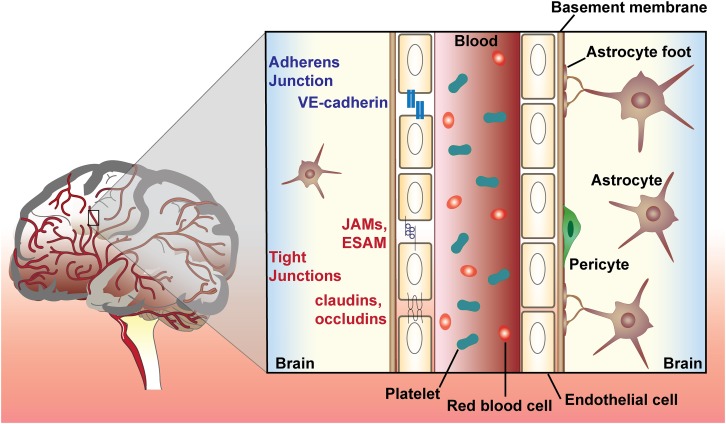
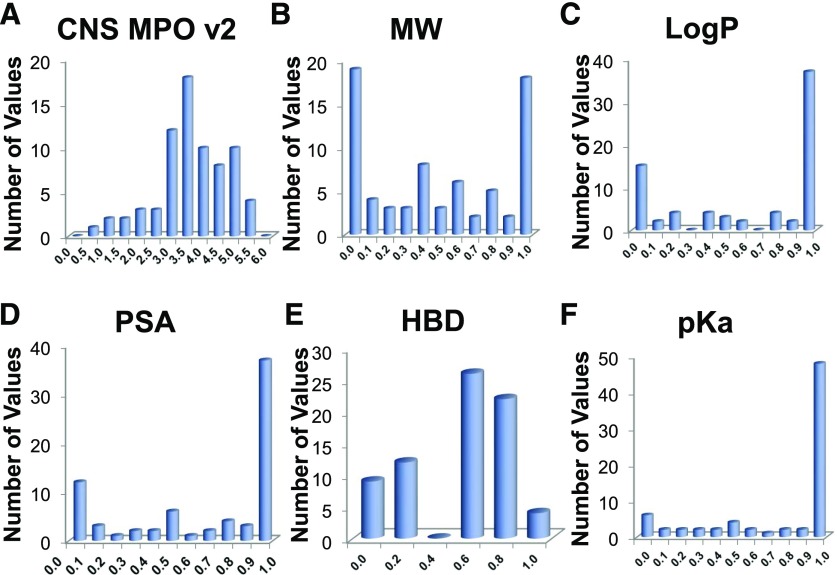
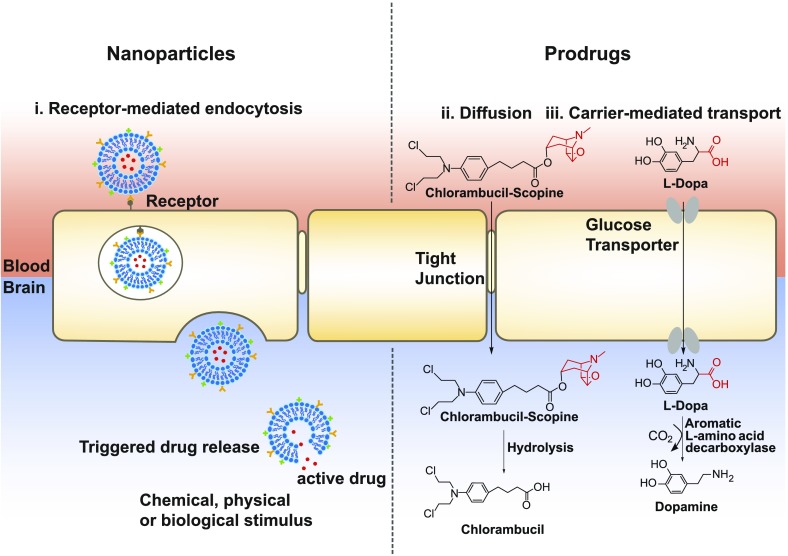
Glioblastoma multiforme (GBM), the most common and aggressive primary brain tumor, has a high mortality rate despite extensive efforts to develop new treatments. GBM exhibits both intra- and intertumor heterogeneity, lending to resistance and eventual tumor recurrence. Large-scale genomic and proteomic analysis of GBM tumors has uncovered potential drug targets. Effective and "druggable" targets must be validated to embark on a robust medicinal chemistry campaign culminating in the discovery of clinical candidates. Here, we review recent developments in GBM drug discovery and delivery. To identify GBM drug targets, we performed extensive bioinformatics analysis using data from The Cancer Genome Atlas project. We discovered 20 genes, BOC, CLEC4GP1, ELOVL6, EREG, ESR2, FDCSP, FURIN, FUT8-AS1, GZMB, IRX3, LITAF, NDEL1, NKX3-1, PODNL1, PTPRN, QSOX1, SEMA4F, TH, VEGFC, and C20orf166AS1 that are overexpressed in a subpopulation of GBM patients and correlate with poor survival outcomes. Importantly, nine of these genes exhibit higher expression in GBM versus low-grade glioma and may be involved in disease progression. In this review, we discuss these proteins in the context of GBM disease progression. We also conducted computational multi-parameter optimization to assess the blood-brain barrier (BBB) permeability of small molecules in clinical trials for GBM treatment. Drug delivery in the context of GBM is particularly challenging because the BBB hinders small molecule transport. Therefore, we discuss novel drug delivery methods, including nanoparticles and prodrugs. Given the aggressive nature of GBM and the complexity of targeting the central nervous system, effective treatment options are a major unmet medical need. Identification and validation of biomarkers and drug targets associated with GBM disease progression present an exciting opportunity to improve treatment of this devastating disease.
Copyright © 2018 by The Author(s).
Figures
References
-
- Abadeer NS, Murphy CJ. (2016) Recent progress in cancer thermal therapy using gold nanoparticles. J Phys Chem C 120:4691–4716.
-
- Abate-Shen C, Banach-Petrosky WA, Sun X, Economides KD, Desai N, Gregg JP, Borowsky AD, Cardiff RD, Shen MM. (2003) Nkx3.1; Pten mutant mice develop invasive prostate adenocarcinoma and lymph node metastases. Cancer Res 63:3886–3890. - PubMed
-
- Ahluwalia MS, Papadantonakis N, Alva Venur V, Schilero C, Peereboom DM, Stevens G, Rosenfeld S, Vogelbaum MA, Elson P, Nixon AB, et al. (2015) Phase II trial of dovitinib in recurrent glioblastoma. J Clin Oncol 33:2050.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
