

Overactivity of Alternative Pathway Convertases in Patients With Complement-Mediated Renal Diseases
- PMID: 29670616
- PMCID: PMC5893837
- DOI: 10.3389/fimmu.2018.00612
Overactivity of Alternative Pathway Convertases in Patients With Complement-Mediated Renal Diseases
Abstract
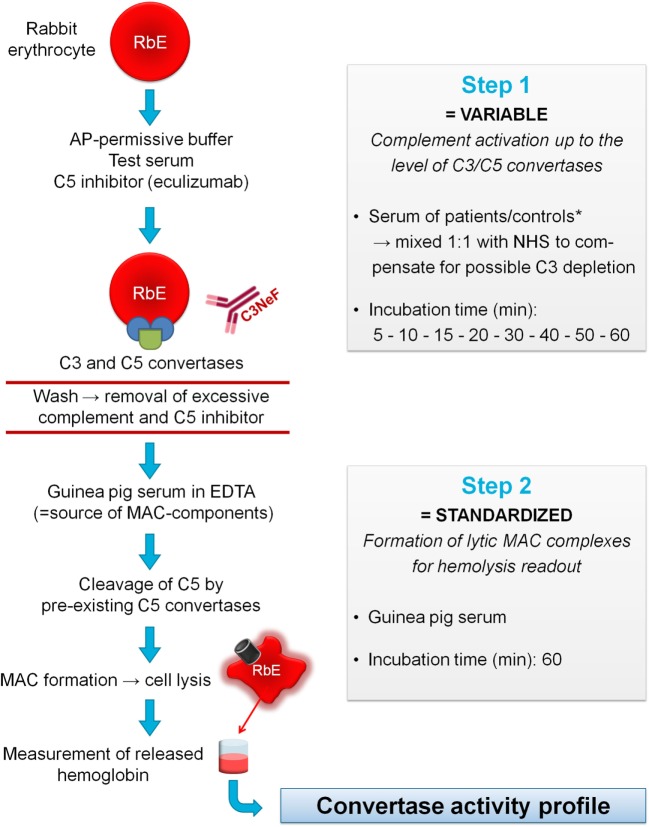
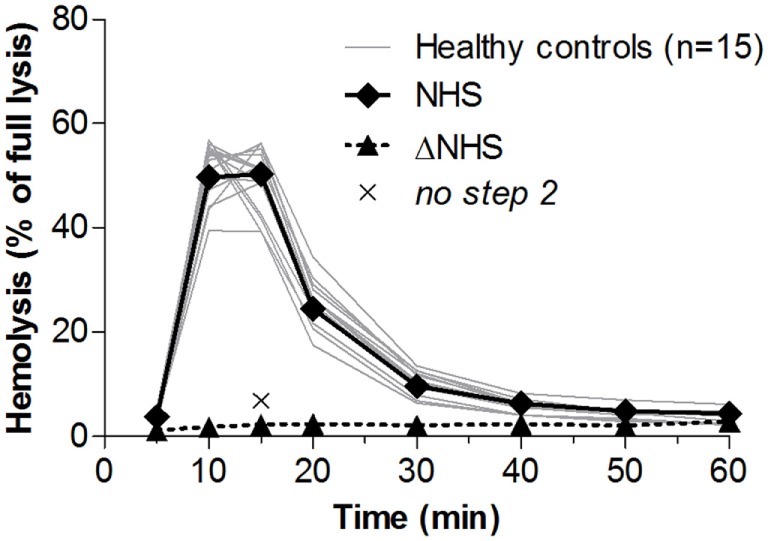
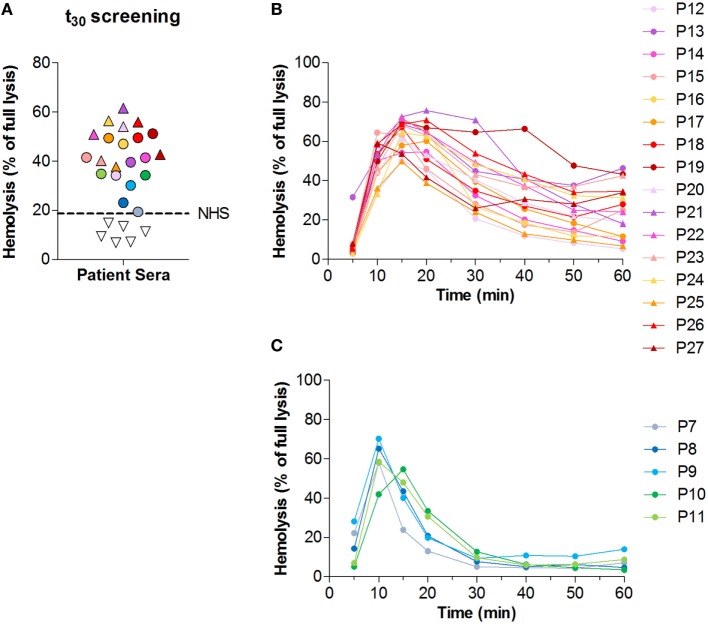
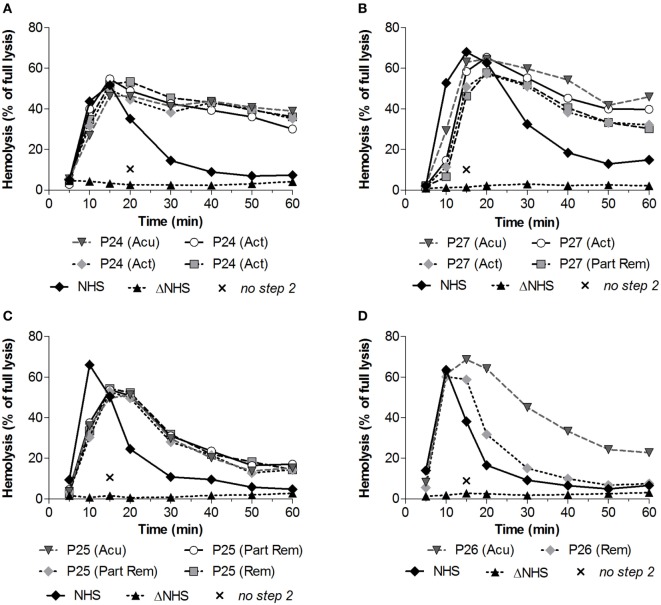
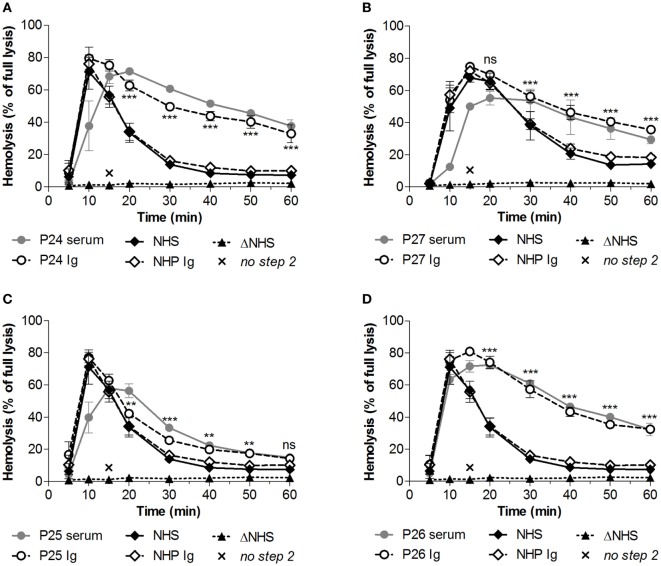
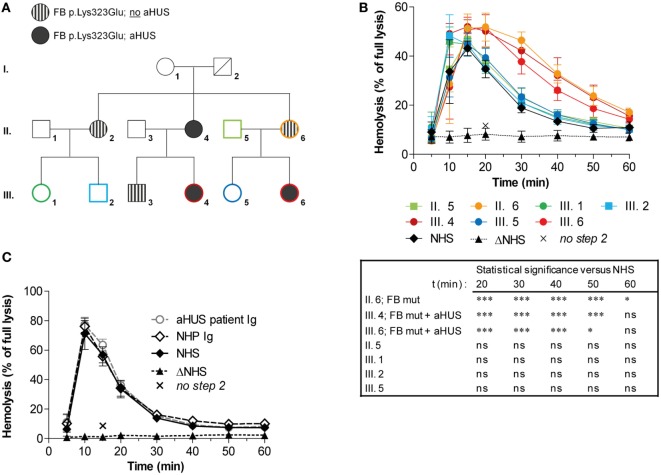
Overactivation of the alternative pathway of the complement system is associated with the renal diseases atypical hemolytic uremic syndrome (aHUS) and C3 glomerulopathy (C3G). C3 nephritic factors (C3NeF) play an important role in C3G pathogenesis by stabilizing the key enzymatic complex of complement, the C3 convertase. However, the reliability of assays detecting these autoantibodies is limited. Therefore, in this study, we validated and optimized a prototype hemolytic method for robust detection and characterization of factors causing convertase overactivity in large patient cohorts. The assay assesses convertase activity directly in the physiological milieu of serum and therefore is not restricted to detection of stabilizing autoantibodies such as C3NeF but may also reveal genetic variants resulting in prolonged convertase activity. We first defined clear cutoff values based on convertase activity in healthy controls. Next, we evaluated 27 C3G patient samples and found 16 positive for prolonged convertase activity, indicating the presence of factors influencing convertase stability. In three patients, the overactive convertase profile was persistent over disease course while in another patient the increased stability normalized in remission. In all these four patients, the convertase-stabilizing activity resided in the purified immunoglobulin (Ig) fraction, demonstrating the autoantibody nature. By contrast, the Igs of a familial aHUS patient carrying the complement factor B mutation p.Lys323Glu did not reveal convertase stabilization. However, in serum prolonged convertase activity was observed and segregated with the mutation in both affected and unaffected family members. In conclusion, we present a robust and reliable method for the detection, characterization, and evaluation over time of factors prolonging convertase activity (C3NeF or certain mutations) in patient cohorts. This assay may provide new insights in disease pathogenesis and may contribute to the development of more personalized treatment strategies.
Keywords: C3 glomerulopathy; C3 nephritic factor; alternative pathway; atypical hemolytic uremic syndrome; complement factor B mutation; complement system; convertase.
Figures
Similar articles
-
Different Aspects of Classical Pathway Overactivation in Patients With C3 Glomerulopathy and Immune Complex-Mediated Membranoproliferative Glomerulonephritis.Front Immunol. 2021 Aug 11;12:715704. doi: 10.3389/fimmu.2021.715704. eCollection 2021. Front Immunol. 2021. PMID: 34456924 Free PMC article.
-
Functional Hemolytic Test for Complement Alternative Pathway Convertase Activity.Methods Mol Biol. 2021;2227:83-96. doi: 10.1007/978-1-0716-1016-9_8. Methods Mol Biol. 2021. PMID: 33847933
-
Novel Assays to Distinguish Between Properdin-Dependent and Properdin-Independent C3 Nephritic Factors Provide Insight Into Properdin-Inhibiting Therapy.Front Immunol. 2019 Jun 17;10:1350. doi: 10.3389/fimmu.2019.01350. eCollection 2019. Front Immunol. 2019. PMID: 31263464 Free PMC article.
-
Autoantibodies to complement components in C3 glomerulopathy and atypical hemolytic uremic syndrome.Immunol Lett. 2014 Aug;160(2):163-71. doi: 10.1016/j.imlet.2014.01.014. Epub 2014 Feb 1. Immunol Lett. 2014. PMID: 24491679 Review.
-
Autoimmune abnormalities of the alternative complement pathway in membranoproliferative glomerulonephritis and C3 glomerulopathy.Pediatr Nephrol. 2019 Aug;34(8):1311-1323. doi: 10.1007/s00467-018-3989-0. Epub 2018 Jun 9. Pediatr Nephrol. 2019. PMID: 29948306 Review.
Cited by
-
Acquired drivers of C3 glomerulopathy.Clin Kidney J. 2025 Jan 27;18(3):sfaf022. doi: 10.1093/ckj/sfaf022. eCollection 2025 Mar. Clin Kidney J. 2025. PMID: 40052168 Free PMC article. Review.
-
Modeling C3 glomerulopathies: C3 convertase regulation on an extracellular matrix surface.Front Immunol. 2023 Jan 18;13:1073802. doi: 10.3389/fimmu.2022.1073802. eCollection 2022. Front Immunol. 2023. PMID: 36846022 Free PMC article.
-
Nephritic Factors: An Overview of Classification, Diagnostic Tools and Clinical Associations.Front Immunol. 2019 Apr 24;10:886. doi: 10.3389/fimmu.2019.00886. eCollection 2019. Front Immunol. 2019. PMID: 31068950 Free PMC article. Review.
-
Long-term follow-up including extensive complement analysis of a pediatric C3 glomerulopathy cohort.Pediatr Nephrol. 2022 Mar;37(3):601-612. doi: 10.1007/s00467-021-05221-6. Epub 2021 Sep 2. Pediatr Nephrol. 2022. PMID: 34476601 Free PMC article.
-
Challenges in diagnostic testing of nephritic factors.Front Immunol. 2022 Nov 14;13:1036136. doi: 10.3389/fimmu.2022.1036136. eCollection 2022. Front Immunol. 2022. PMID: 36451820 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous