

Neuroimaging of Meckel's cave in normal and disease conditions
- PMID: 29671218
- PMCID: PMC6108963
- DOI: 10.1007/s13244-018-0604-7
Neuroimaging of Meckel's cave in normal and disease conditions
Abstract
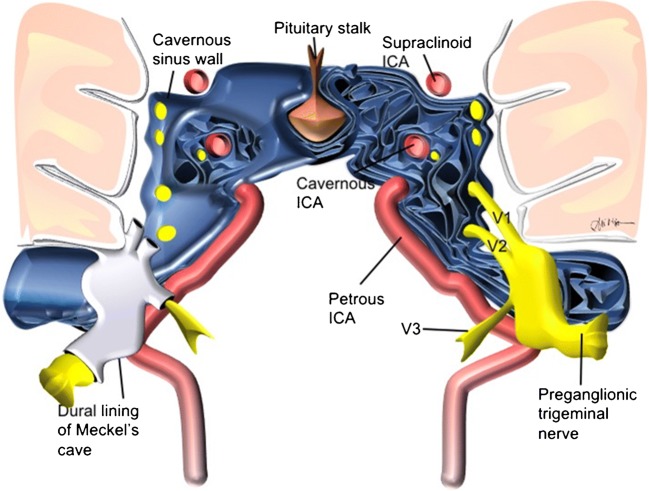
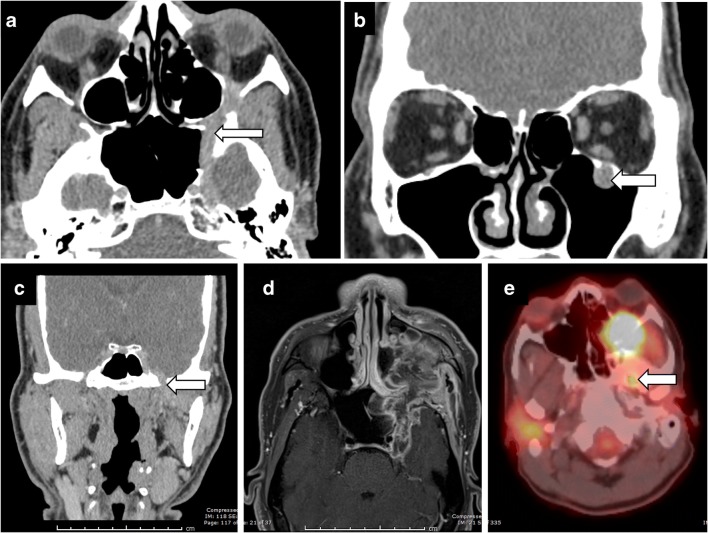
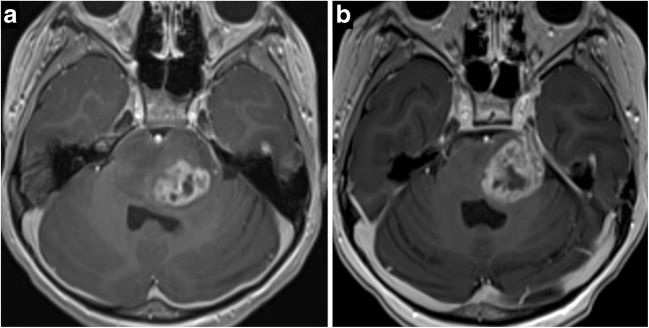
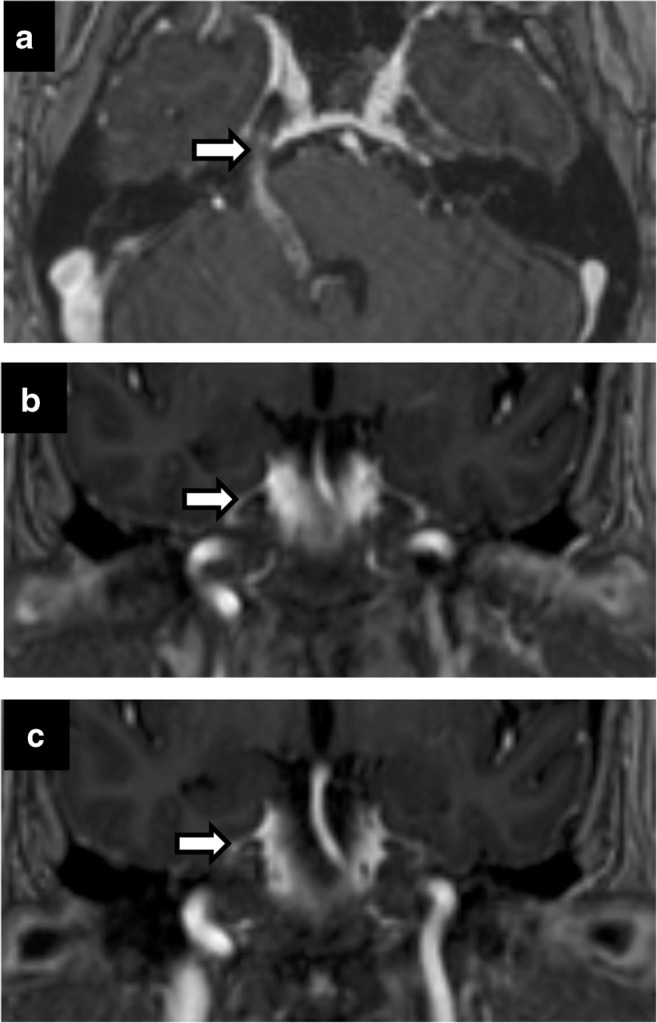
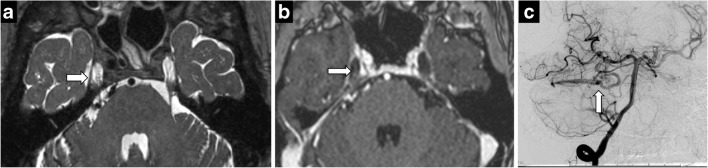
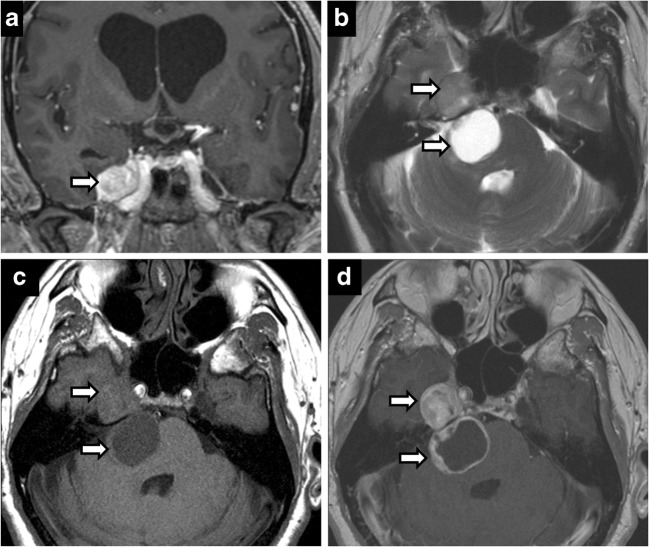
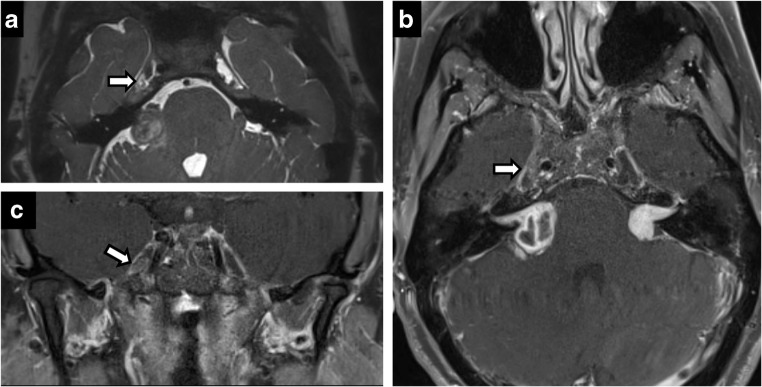
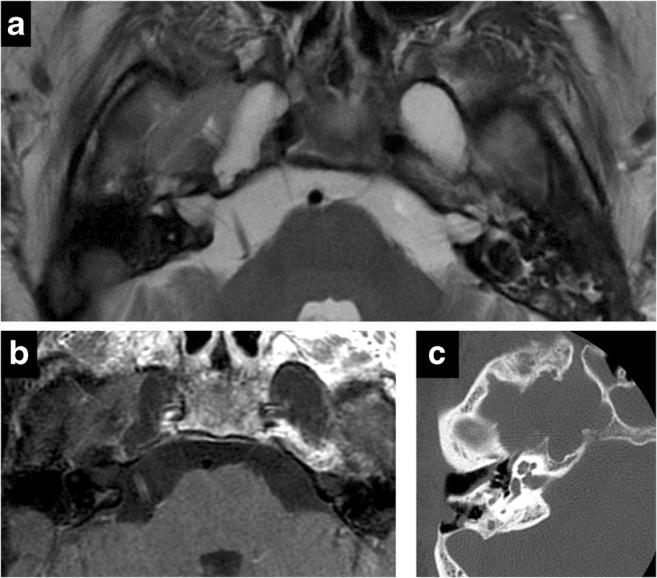
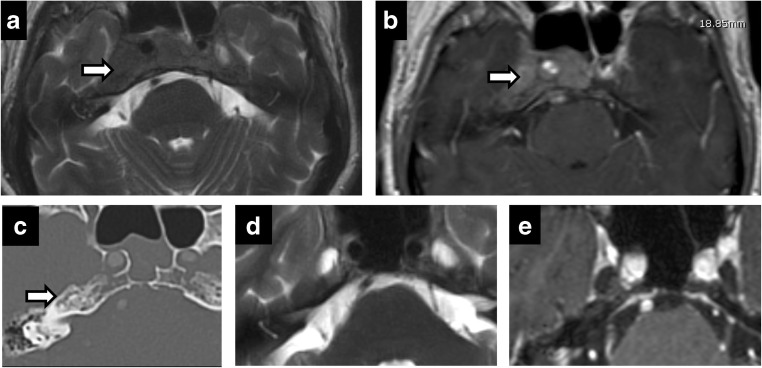
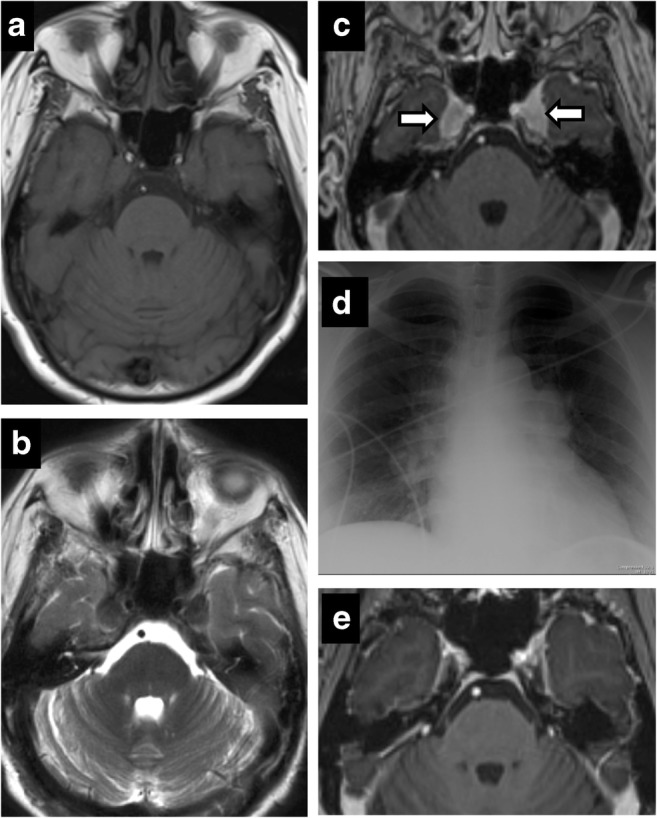
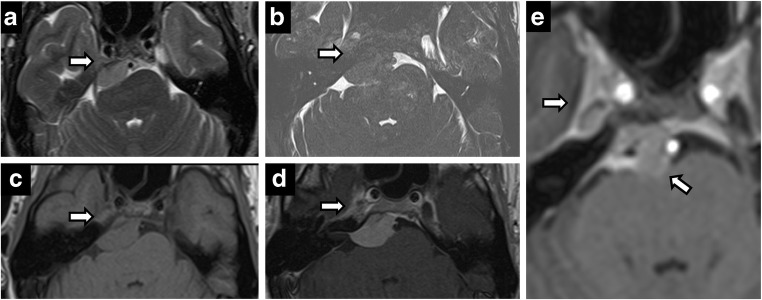
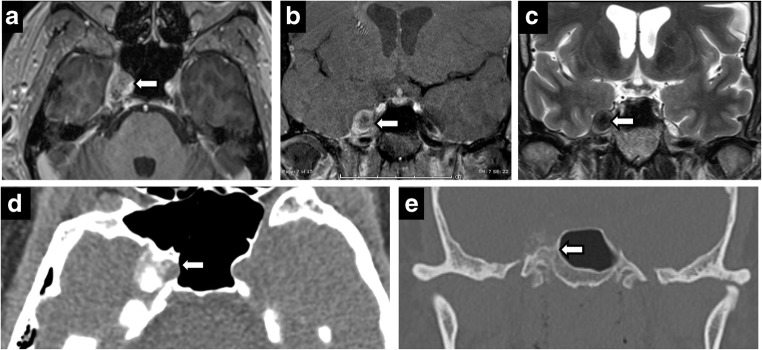
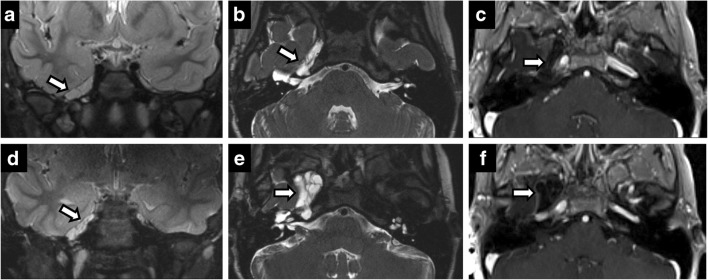
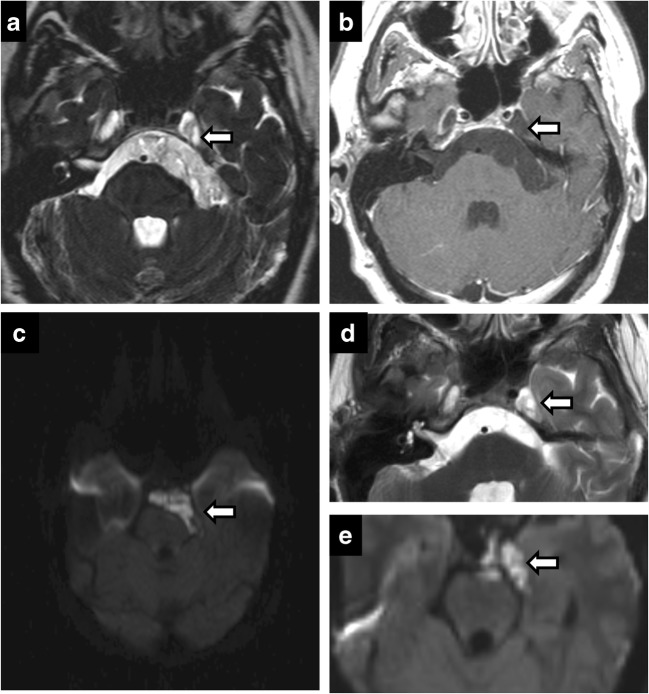
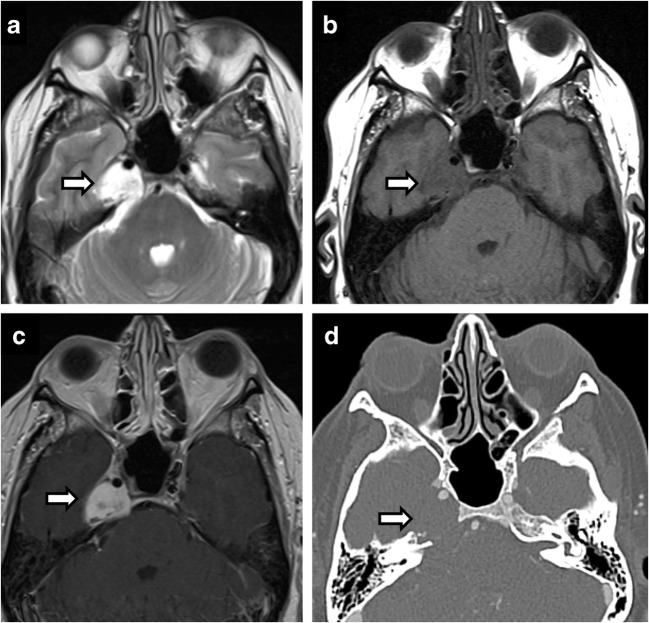
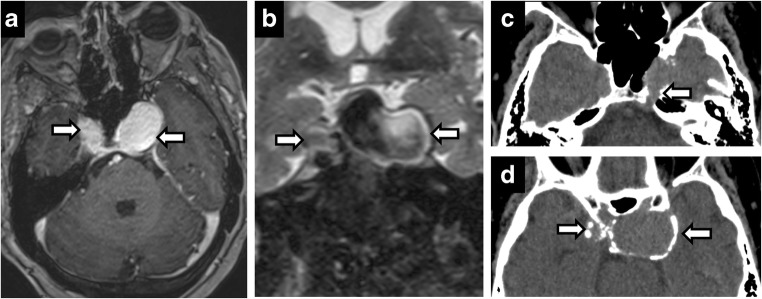
Meckel's cave is a dural recess in the posteromedial portion of the middle cranial fossa that acts as a conduit for the trigeminal nerve between the prepontine cistern and the cavernous sinus, and houses the Gasserian ganglion and proximal rootlets of the trigeminal nerve. It serves as a major pathway in perineural spread of pathologies such as head and neck neoplasms, automatically upstaging tumours, and is a key structure to assess in cases of trigeminal neuralgia. The purpose of this pictorial review is threefold: (1) to review the normal anatomy of Meckel's cave; (2) to describe imaging findings that identify disease involving Meckel's cave; (3) to present case examples of trigeminal and non-trigeminal processes affecting Meckel's cave.
Teaching points: • Meckel's cave contains the trigeminal nerve between prepontine cistern and cavernous sinus. • Assessment is essential for perineural spread of disease and trigeminal neuralgia. • Key imaging: neural enhancement, enlargement, perineural fat/CSF effacement, skull base foraminal changes.
Keywords: Meckel’s cave; Neuralgia; Perineural; Skull base; Trigeminal.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
