

Gallstone disease and increased risk of mortality: Two large prospective studies in US men and women
- PMID: 29671893
- PMCID: PMC9015210
- DOI: 10.1111/jgh.14264
Gallstone disease and increased risk of mortality: Two large prospective studies in US men and women
Abstract
Background and aim: Gallstone disease has been related to a higher prevalence and incidence of chronic conditions, such as dyslipidemia, obesity, and cardiovascular disease (CVD). However, limited data are available regarding whether gallstone disease is related to mortality.
Methods: We examined the relationship of a history of gallstone disease and risk of death, using Cox proportional hazards regression analysis, among 86 030 women from the Nurses' Health Study and 43 949 men from the Health Professionals Follow-up Study.
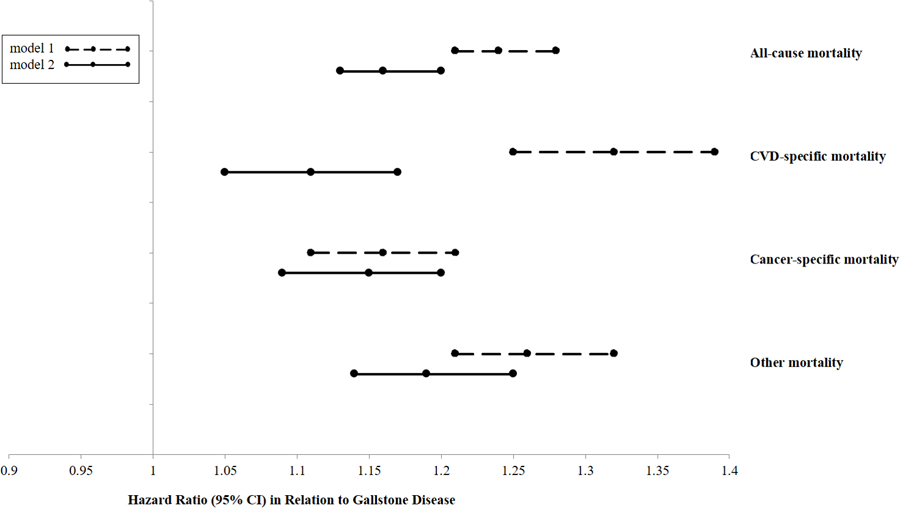
Results: During the up-to 32 years of follow-up, 34 011 all-cause deaths were confirmed, of which 8138 were CVD deaths and 12 173 were cancer deaths. For the participants with a history of gallstone disease compared with those without, the hazard ratio of total mortality was 1.16 (95% confidence interval 1.13, 1.20), of CVD mortality 1.11 (1.05, 1.17), of cancer mortality 1.15 (1.09, 1.20), and of other mortality 1.19 (1.14, 1.25) from a pooled-analysis of women and men (all P < 0.001). The multi-adjusted associations between gallstone disease and total mortality persisted among women and men, and among participants with various risk profiles including the different status of body mass index, hormone therapy use, diabetes, hypertension, and hypercholesterolemia (all P for interaction ≥ 0.09).
Conclusion: These data suggest that gallstone disease is associated with a higher risk of total mortality and disease-specific mortality, including CVD and cancer mortality, independent of various traditional risk factors.
Keywords: cohort studies; gallstone disease; mortality.
© 2018 Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
Figures
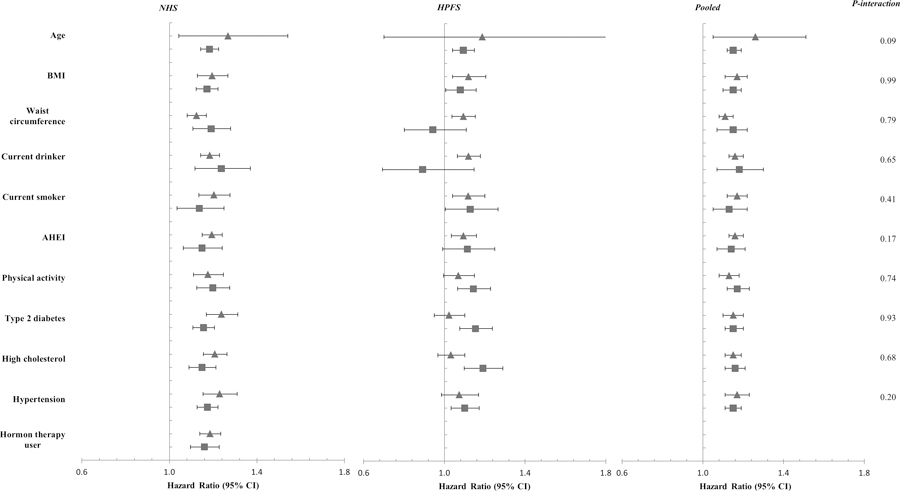
 indicates a lower level of the stratifying variable, i.e., age < 55 years, BMI < 30 kg/m2, weight circumference, physical activity, and AHEI score was lower than the cohort-specific median, nondrinker, nonsmoker, free of type 2 diabetes, high cholesterol, or hypertension, and hormone therapy nonuser in women;
indicates a lower level of the stratifying variable, i.e., age < 55 years, BMI < 30 kg/m2, weight circumference, physical activity, and AHEI score was lower than the cohort-specific median, nondrinker, nonsmoker, free of type 2 diabetes, high cholesterol, or hypertension, and hormone therapy nonuser in women;  indicates a higher level of the stratifying variable.
indicates a higher level of the stratifying variable.References
-
- Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet 2006; 368: 230–9. - PubMed
-
- Kratzer W, Mason RA, Kachele V. Prevalence of gallstones in sonographic surveys worldwide. J Clin Ultrasound 1999; 27: 1–7. - PubMed
-
- Stender S, Nordestgaard BG, Tybjaerg-Hansen A. Elevated body mass index as a causal risk factor for symptomatic gallstone disease: a Mendelian randomization study. Hepatology 2013; 58: 2133–41. - PubMed
MeSH terms
Grants and funding
- DK078616/American Heart Association Scientist Development Award
- UM1 CA176726/CA/NCI NIH HHS/United States
- UM1 CA186107/NH/NIH HHS/United States
- DK46200/Shanghai Thousand Talents Program for Distinguished Scholars
- P30 DK046200/DK/NIDDK NIH HHS/United States
- R01 HL35464/NH/NIH HHS/United States
- NIH Office of the Director
- R01 HL071981/HL/NHLBI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
- R01 DK078616/DK/NIDDK NIH HHS/United States
- 7-12-MN-34/United States - Israel Binational Science Foundation Grant
- HL071981/American Diabetes Association
- R01 HL034594/NH/NIH HHS/United States
- Boston Obesity Nutrition Research Center
- R01 DK091718/DK/NIDDK NIH HHS/United States
- 0730094N/NH/NIH HHS/United States
- R21 HL126024/HL/NHLBI NIH HHS/United States
- R01 HL034594/HL/NHLBI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- 2011036/HL/NHLBI NIH HHS/United States
- U01 DK078616/DK/NIDDK NIH HHS/United States
- R01 DK100383/DK/NIDDK NIH HHS/United States
- UM1 CA167552/NH/NIH HHS/United States
- UM1 CA176726/NH/NIH HHS/United States
- R01 HL035464/HL/NHLBI NIH HHS/United States
- DK100383/American Heart Association Scientist Development Award
- HL034594/American Diabetes Association
- DK091718/American Heart Association Scientist Development Award
- UM1 DK078616/DK/NIDDK NIH HHS/United States
- HL126024/American Diabetes Association
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
