

Pruning of the Pulmonary Vasculature in Asthma. The Severe Asthma Research Program (SARP) Cohort
- PMID: 29672122
- PMCID: PMC6034125
- DOI: 10.1164/rccm.201712-2426OC
Pruning of the Pulmonary Vasculature in Asthma. The Severe Asthma Research Program (SARP) Cohort
Abstract
Rationale: Loss of the peripheral pulmonary vasculature, termed vascular pruning, is associated with disease severity in patients with chronic obstructive pulmonary disease.
Objectives: To determine if pulmonary vascular pruning is associated with asthma severity and exacerbations.
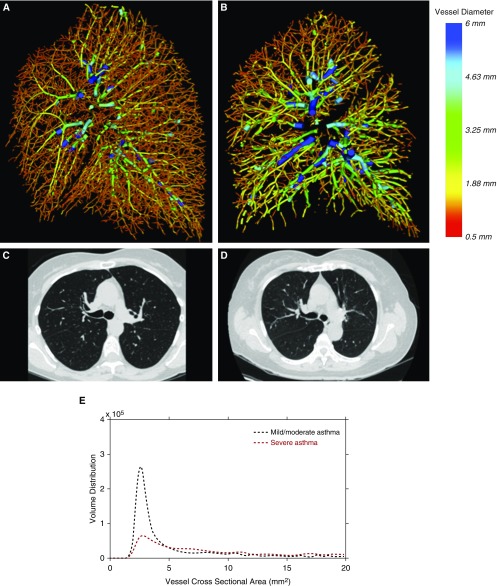
Methods: We measured the total pulmonary blood vessel volume (TBV) and the blood vessel volume of vessels less than 5 mm2 in cross-sectional area (BV5) and of vessels less than 10 mm2 (BV10) in cross-sectional area on noncontrast computed tomographic scans of participants from the Severe Asthma Research Program. Lower values of the BV5 to TBV ratio (BV5/TBV) and the BV10 to TBV ratio (BV10/TBV) represented vascular pruning (loss of the peripheral pulmonary vasculature).
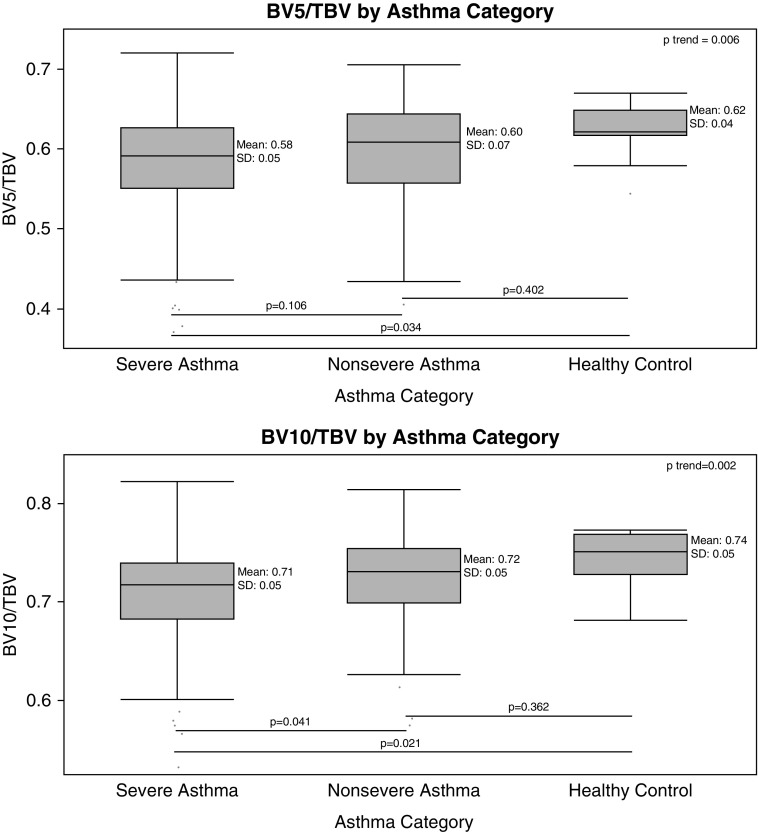
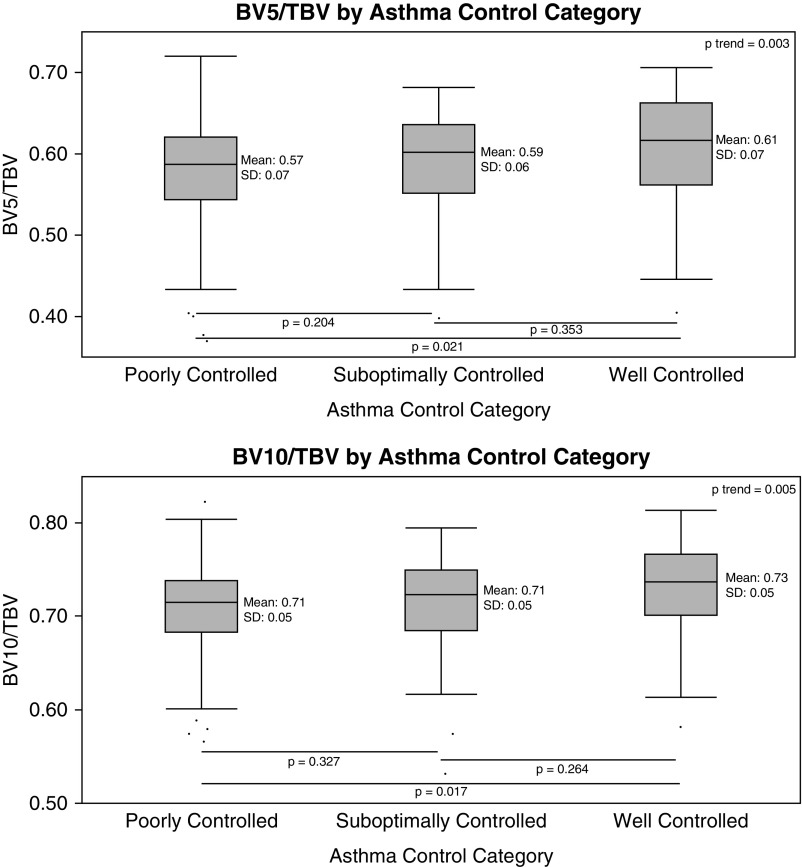
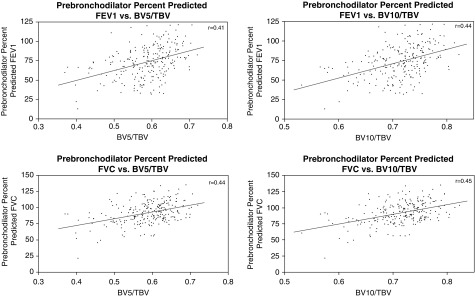
Measurements and main results: Compared with healthy control subjects, patients with severe asthma had more pulmonary vascular pruning. Among those with asthma, those with poor asthma control had more pruning than those with well-controlled disease. Pruning of the pulmonary vasculature was also associated with lower percent predicted FEV1 and FVC, greater peripheral and sputum eosinophilia, and higher BAL serum amyloid A/lipoxin A4 ratio but not with low-attenuation area or with sputum neutrophilia. Compared with individuals with less pruning, individuals with the most vascular pruning had 150% greater odds of reporting an asthma exacerbation (odds ratio, 2.50; confidence interval, 1.05-5.98; P = 0.039 for BV10/TBV) and reported 45% more asthma exacerbations during follow-up (incidence rate ratio, 1.45; confidence interval, 1.02-2.06; P = 0.036 for BV10/TBV).
Conclusions: Pruning of the peripheral pulmonary vasculature is associated with asthma severity, control, and exacerbations, and with lung function and eosinophilia.
Keywords: eosinophilia; pruning; pulmonary vascular; severe asthma.
Figures
Comment in
-
The Matter of the Lung: Quantification of Vascular Substance in Asthma.Am J Respir Crit Care Med. 2018 Jul 1;198(1):1-2. doi: 10.1164/rccm.201804-0804ED. Am J Respir Crit Care Med. 2018. PMID: 29882680 No abstract available.
References
-
- Cordasco EM, Beerel FR, Vance JW, Wende RW, Toffolo RR. Newer aspects of the pulmonary vasculature in chronic lung disease. A comparative study. Angiology. 1968;19:399–407. - PubMed
-
- Hale KA, Niewoehner DE, Cosio MG. Morphologic changes in the muscular pulmonary arteries: relationship to cigarette smoking, airway disease, and emphysema. Am Rev Respir Dis. 1980;122:273–278. - PubMed
-
- Minai OA, Chaouat A, Adnot S. Pulmonary hypertension in COPD: epidemiology, significance, and management: pulmonary vascular disease: the global perspective. Chest. 2010;137(Suppl. 6):39S–51S. - PubMed
-
- Wright JL, Lawson L, Paré PD, Hooper RO, Peretz DI, Nelems JM, et al. The structure and function of the pulmonary vasculature in mild chronic obstructive pulmonary disease. The effect of oxygen and exercise. Am Rev Respir Dis. 1983;128:702–707. - PubMed
Publication types
MeSH terms
Grants and funding
- T32 HL007633/HL/NHLBI NIH HHS/United States
- UL1 TR000427/TR/NCATS NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- K23 HL136905/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- R01 HL122531/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- U10 HL109172/HL/NHLBI NIH HHS/United States
- U10 HL064313/HL/NHLBI NIH HHS/United States
- U10 HL109257/HL/NHLBI NIH HHS/United States
- K23 HL114735/HL/NHLBI NIH HHS/United States
- R01 HL116931/HL/NHLBI NIH HHS/United States
- K23 AI125785/AI/NIAID NIH HHS/United States
- UL1 TR002373/TR/NCATS NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- U10 HL109086/HL/NHLBI NIH HHS/United States
- U10 HL109168/HL/NHLBI NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- U10 HL109152/HL/NHLBI NIH HHS/United States
- U10 HL109146/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
