

Nocturnal swallowing and arousal threshold in individuals with chronic spinal cord injury
- PMID: 29672224
- PMCID: PMC6734058
- DOI: 10.1152/japplphysiol.00641.2017
Nocturnal swallowing and arousal threshold in individuals with chronic spinal cord injury
Abstract
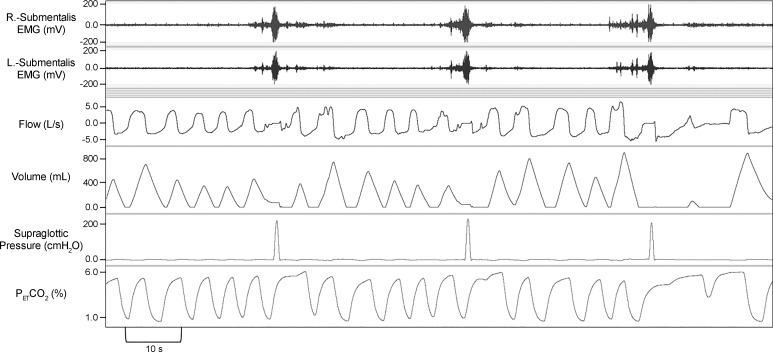
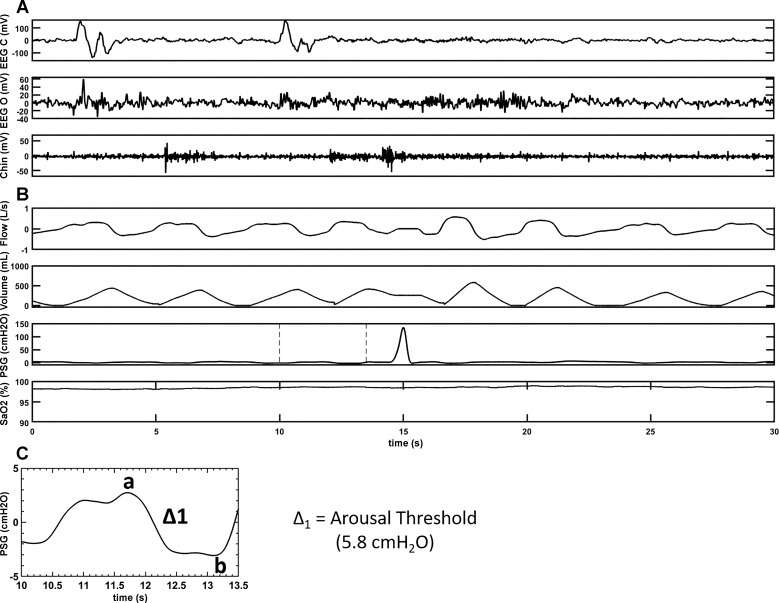
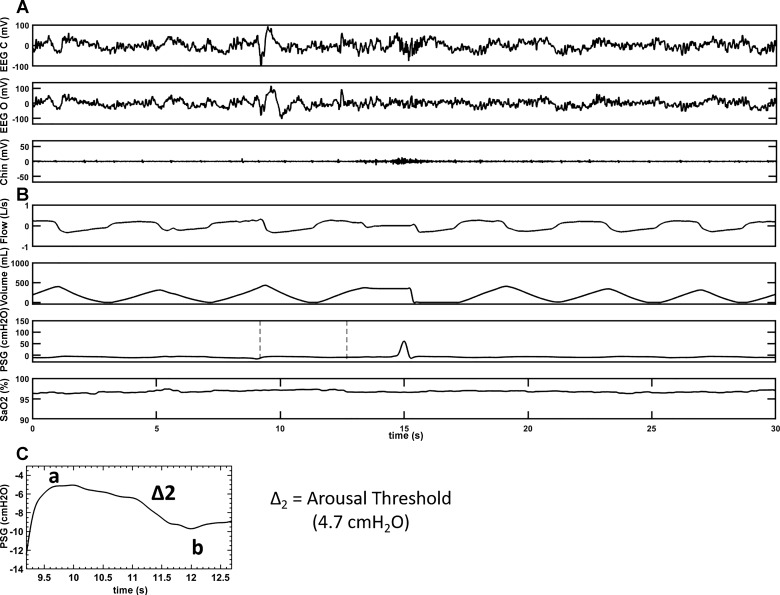
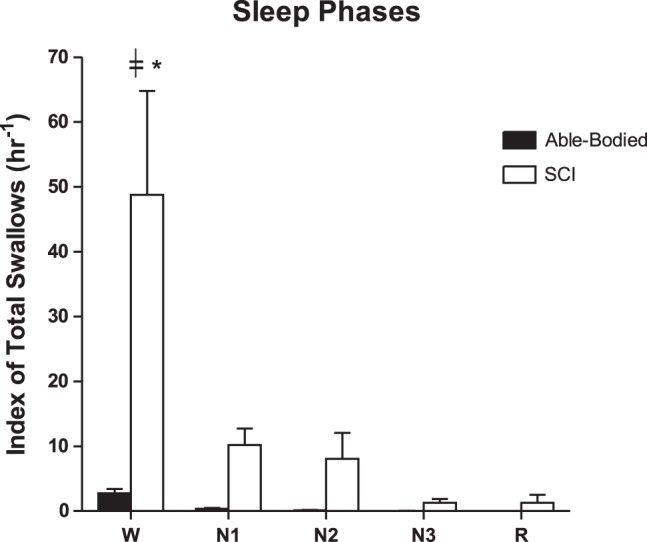
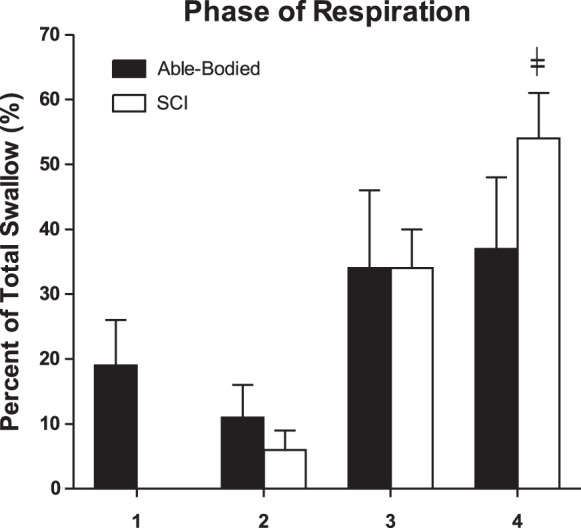
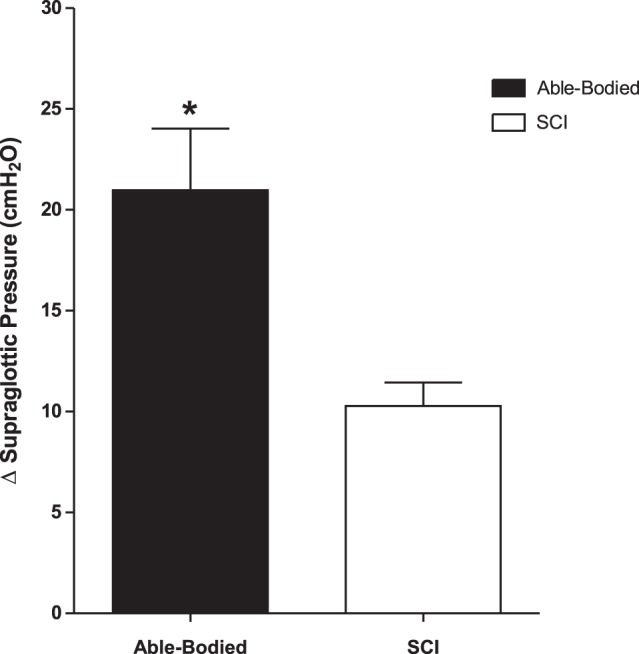
Respiratory complications are potential causes of death in patients with spinal cord injury (SCI). Nocturnal swallowing could be related to transient arousals and could lead to fragmented sleep in SCI patients. However, the impact of nocturnal swallowing on breathing and sleep physiology in SCI is unknown. The objectives of this study were 1) to determine whether nocturnal swallowing is more common in SCI than in able-bodied (AB) subjects, 2) to determine the role of nocturnal swallowing on arousal threshold (ArTh) in SCI individuals with sleep-disordered breathing (SDB), and 3) to determine the effect of continuous positive airway pressure (CPAP) treatment on nocturnal swallowing. A total of 16 SCI and 13 AB subjects with SDB completed in-laboratory polysomnography with a pharyngeal catheter. A swallowing event (SW) was defined as a positive spike in pharyngeal pressure and was used to calculate the swallow index (SI) defined as a number of SW/total sleep time. Each SW was assessed for a relationship to the sleep stages and respiratory cycle phases, and associated arousals and ArTh were calculated. SI was higher in the SCI group compared with AB subjects during wake and different sleep stages ( P < 0.05). SWs were found to be significantly higher in the late expiratory phase in the group with SCI compared with the other respiratory phases and were eliminated by CPAP ( P < 0.05). ArTh for the subjects with SCI was significantly lower ( P < 0.05) compared with the AB subjects. Nocturnal swallowing is more common in SCI than in AB individuals who have SDB, particularly during the expiratory phase. The ArTh is significantly lower in SCI (indicating increased arousal propensity), which may contribute to the mechanism of sleep disturbances in SCI. NEW & NOTEWORTHY Nocturnal swallowing is common in patients with chronic spinal cord injury (SCI) and is associated with frequent arousals from sleep. The lower arousal threshold during sleep in SCI may contribute to the mechanism of sleep disturbances that are commonly found in cervical and high thoracic SCI. Continuous positive airway pressure may play a therapeutic role in alleviating nocturnal swallowing, which may contribute to reduced risk of aspiration.
Keywords: arousal; arousal threshold; sleep; sleep-disordered breathing; spinal cord injury; swallowing.
Figures
Similar articles
-
Sleep-Disordered Breathing and Spinal Cord Injury: A State-of-the-Art Review.Chest. 2019 Feb;155(2):438-445. doi: 10.1016/j.chest.2018.10.002. Epub 2018 Oct 12. Chest. 2019. PMID: 30321507 Free PMC article. Review.
-
Sleep disordered breathing in chronic spinal cord injury.J Clin Sleep Med. 2014 Jan 15;10(1):65-72. doi: 10.5664/jcsm.3362. J Clin Sleep Med. 2014. PMID: 24426822 Free PMC article.
-
New insights into the timing and potential mechanisms of respiratory-induced cortical arousals in obstructive sleep apnea.Sleep. 2018 Nov 1;41(11):zsy160. doi: 10.1093/sleep/zsy160. Sleep. 2018. PMID: 30137568 Free PMC article.
-
Sleep disordered breathing induced by cervical spinal cord injury and effect of adenosine A1 receptors modulation in rats.J Appl Physiol (1985). 2019 Dec 1;127(6):1668-1676. doi: 10.1152/japplphysiol.00563.2019. Epub 2019 Oct 10. J Appl Physiol (1985). 2019. PMID: 31600096
-
The impact of spinal cord injury on breathing during sleep.Respir Physiol Neurobiol. 2013 Sep 15;188(3):344-54. doi: 10.1016/j.resp.2013.06.009. Epub 2013 Jun 17. Respir Physiol Neurobiol. 2013. PMID: 23791824 Free PMC article. Review.
Cited by
-
Impact Of Spinal Cord Injury On Sleep: Current Perspectives.Nat Sci Sleep. 2019 Oct 15;11:219-229. doi: 10.2147/NSS.S197375. eCollection 2019. Nat Sci Sleep. 2019. PMID: 31686935 Free PMC article.
-
Tetraplegia is associated with increased hypoxic ventilatory response during nonrapid eye movement sleep.Physiol Rep. 2022 Sep;10(17):e15455. doi: 10.14814/phy2.15455. Physiol Rep. 2022. PMID: 36065854 Free PMC article.
-
Effect of Zolpidem on nocturnal arousals and susceptibility to central sleep apnea.Sleep Breath. 2023 Mar;27(1):173-180. doi: 10.1007/s11325-022-02593-3. Epub 2022 Mar 14. Sleep Breath. 2023. PMID: 35286569 Free PMC article. Clinical Trial.
-
Mirtazapine reduces susceptibility to hypocapnic central sleep apnea in males with sleep-disordered breathing: a pilot study.J Appl Physiol (1985). 2021 Jul 1;131(1):414-423. doi: 10.1152/japplphysiol.00838.2020. Epub 2021 Jun 3. J Appl Physiol (1985). 2021. PMID: 34080920 Free PMC article. Clinical Trial.
-
Sleep-Disordered Breathing and Spinal Cord Injury: A State-of-the-Art Review.Chest. 2019 Feb;155(2):438-445. doi: 10.1016/j.chest.2018.10.002. Epub 2018 Oct 12. Chest. 2019. PMID: 30321507 Free PMC article. Review.
References
-
- Berry R, Brooks R, Gamaldo C, Harding S, Marcus C, Vaughn B. The AASM Manual for The Scoring of Sleep and Associated Events: Rules, Terminology And Technical Specifications, Version 2.0. Darien, Illinois: American Academy of Sleep Medicine, 2012, p. 47.
-
- DeVivo MJ, Black KJ, Stover SL. Causes of death during the first 12 years after spinal cord injury. Arch Phys Med Rehabil 74: 248–254, 1993. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical