

Costs and effectiveness of pharmacist-led group medical visits for type-2 diabetes: A multi-center randomized controlled trial
- PMID: 29672567
- PMCID: PMC5908172
- DOI: 10.1371/journal.pone.0195898
Costs and effectiveness of pharmacist-led group medical visits for type-2 diabetes: A multi-center randomized controlled trial
Abstract
Objectives: The effectiveness and costs associated with addition of pharmacist-led group medical visits to standard care for patients with Type-2 Diabetes Mellitus (T2DM) is unknown.
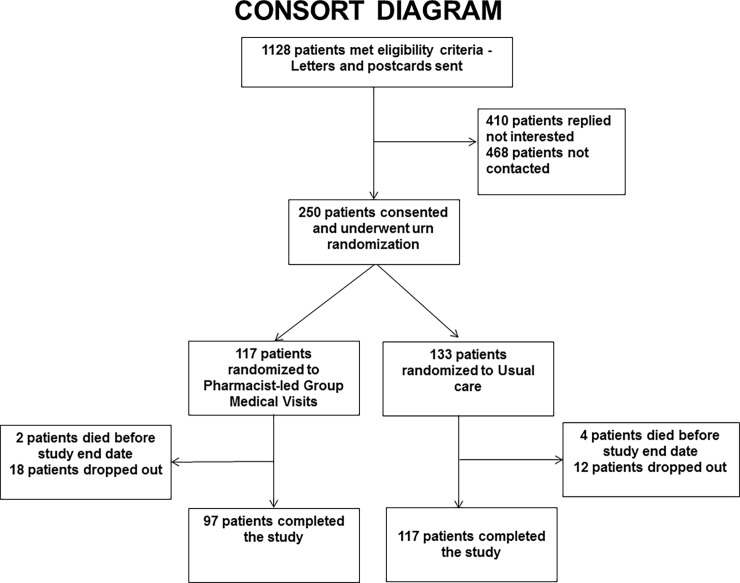
Methods: Randomized-controlled-trial in three US Veteran Health Administration (VHA) Hospitals, where 250 patients with T2DM, HbA1c >7% and either hypertension, active smoking or hyperlipidemia were randomized to either (1) addition of pharmacist-led group-medical-visits or (2) standard care alone for 13 months. Group (4-6 patients) visits consisted of 2-hour, education and comprehensive medication management sessions once weekly for 4 weeks, followed by quarterly visits. Change from baseline in cardiovascular risk estimated by the UKPDS-risk-score, health-related quality-of-life (SF36v) and institutional healthcare costs were compared between study arms.
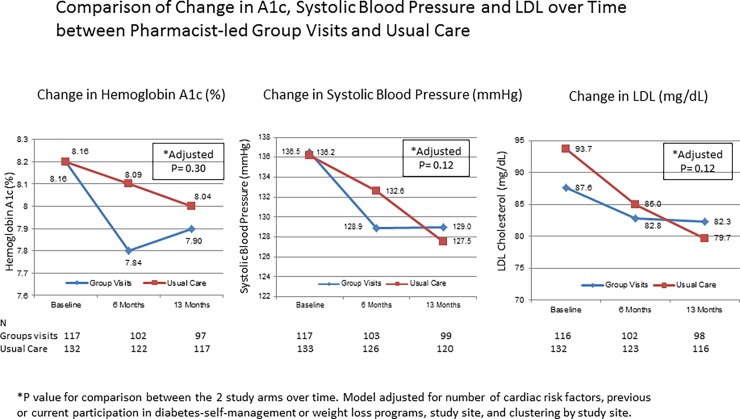
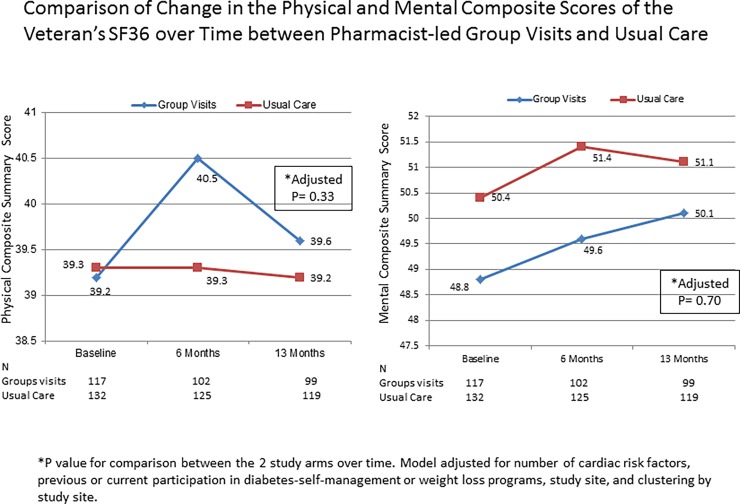
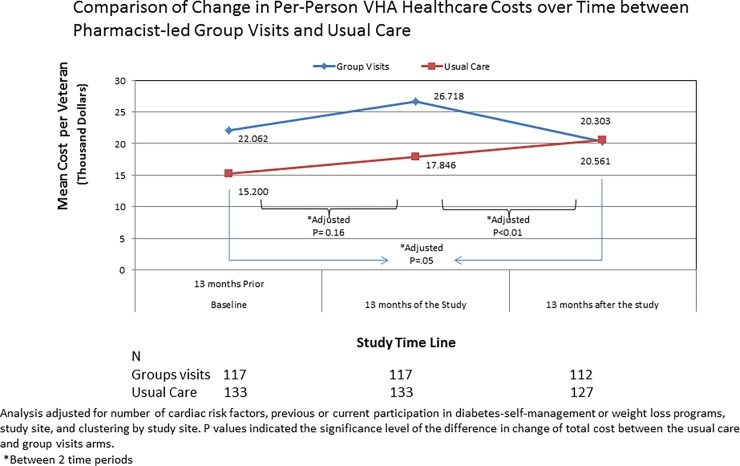
Results: After 13 months, both groups had similar and significant improvements from baseline in UKPDS-risk-score (-0.02 ±0.09 and -0.04 ±0.09, group visit and standard care respectively, adjusted p<0.05 for both); however, there was no significant difference between the study arms (adjusted p = 0.45). There were no significant differences on improvement from baseline in A1c, systolic-blood-pressure, and LDL as well as health-related quality-of-life measures between the study arms. Compared to 13 months prior, the increase in per-person outpatient expenditure from baseline was significantly lower in the group visit versus the standard care arm, both during the study intervention period and at 13-months after study interventions. The overall VHA healthcare costs/person were comparable between the study arms during the study period (p = 0.15); then decreased by 6% for the group visit but increased by 13% for the standard care arm 13 months post-study (p<0.01).
Conclusions: Addition of pharmacist-led group medical visits in T2DM achieved similar improvements from baseline in cardiovascular risk factors than usual care, but with reduction in the healthcare costs in the group visit arm 13 months after completion compared to the steady rise in cost for the usual care arm.
Trial registration: NCT00554671 ClinicalTrials.gov.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control. The Burden of Chronic Diseases and Their Risk Factors: National and State Perspectives 2004 Atlanta: National Center for Chronic Disease Prevention and Health Promotion, 2004.
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133(4):e38–e360. doi: 10.1161/CIR.0000000000000350 . - DOI - PubMed
-
- Gaede P, Vedel P, Larsen N, Jensen GV, Parving H-H, Pedersen O. Multifactorial Intervention and Cardiovascular Disease in patients with type 2 diabetes. New Engl J Med. 2003;348(5):383–93. doi: 10.1056/NEJMoa021778 - DOI - PubMed
-
- The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. New Engl J Med. 2005;353(25):2643–53. doi: 10.1056/NEJMoa052187 - DOI - PMC - PubMed
-
- The CDC Diabetes Cost-effectiveness Group. Cost-effectiveness of intensive glycemic control, intensified hypertension control, and serum cholesterol level reduction for type 2 diabetes. JAMA. 2002;287(19):2542–51. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
