

Intravascular ultrasound assisted sizing in thoracic endovascular aortic repair improves aortic remodeling in Type B aortic dissection
- PMID: 29672613
- PMCID: PMC5908162
- DOI: 10.1371/journal.pone.0196180
Intravascular ultrasound assisted sizing in thoracic endovascular aortic repair improves aortic remodeling in Type B aortic dissection
Abstract
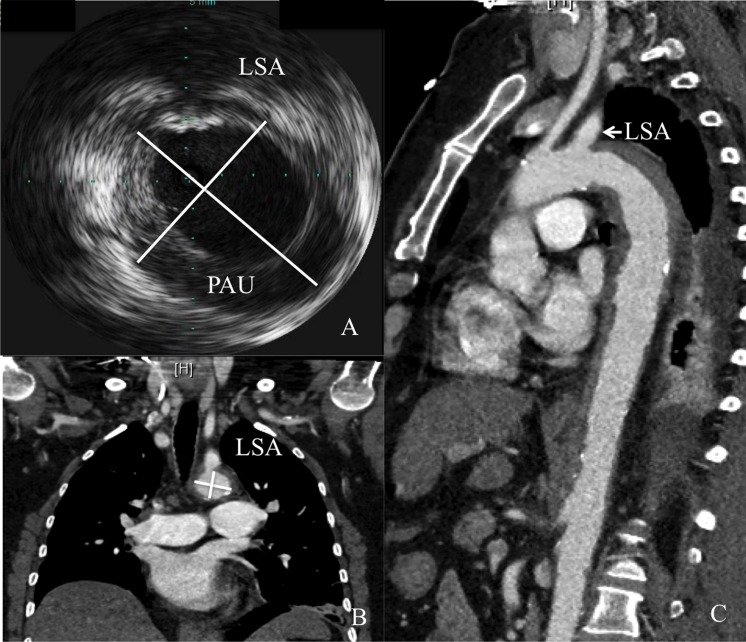
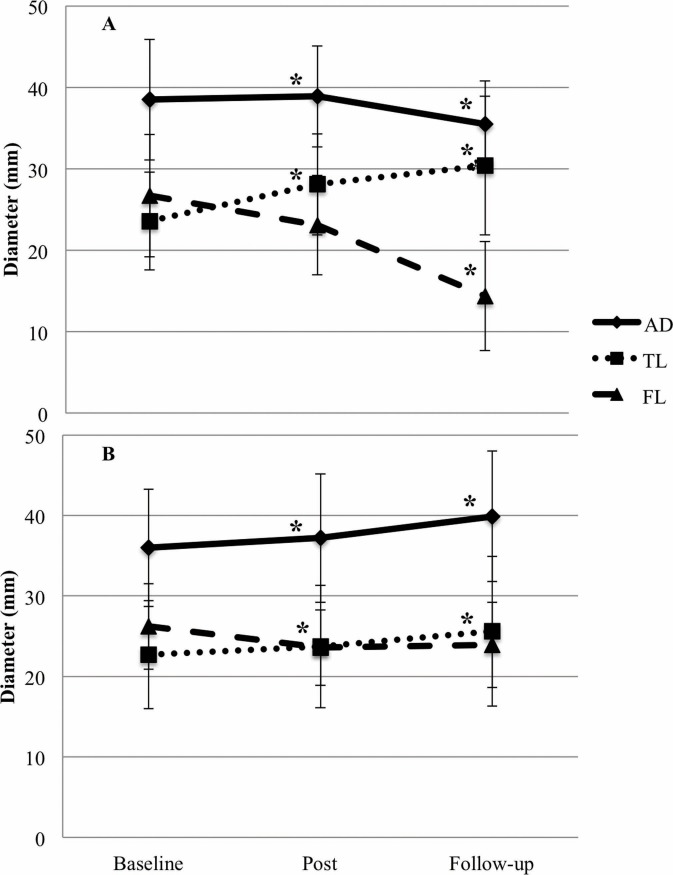
The precise sizing of the stent graft in thoracic endovascular aortic repair (TEVAR) affects aortic remodeling and hence, further outcome. Covering the proximal entry tear is essential for successful treatment of Type B aortic dissection. Intravascular ultrasound (IVUS) enables real-time aortic diameter assessment, and is especially useful when computed tomography (CT) image quality is poor. IVUS, however, is not routinely utilized due to cost inefficiency. We investigated the impact of IVUS-assisted stent graft sizing on aortic remodeling in TEVAR. In this single-center retrospective study we evaluated patients with Type B aortic dissection undergoing both CT and IVUS before TEVAR. We assessed the aortic diameter at the level of the left subclavian artery via both methods before stent implantation and analyzed due to which method the implanted stent graft was chosen, retrospectively. To determine the degrees of aortic remodeling involved, we evaluated true lumen and false lumen diameters, and total aortic remodeling in CT. We analyzed 45 patients with Type B aortic dissection undergoing TEVAR. The mean ages were 66.9±10.0 years fo0072 IVUS (n = 20) and 62.3±14.2 years for CT-assisted TEVAR (n = 25; p = 0.226). The follow-up time for both groups did not differ between the two groups (IVUS: 22.9±23.1 months, CT: 25.6±23.0 months; p = 0.700). While both methods were associated with advantages regarding aortic remodeling, IVUS-assisted sizing yielded a greater increase in true lumen (30.4±6.2 vs. 25.6±5.3; p = 0.008) and reductions in false lumen (14.4±8.5 vs. 23.9±9.3; p = 0.001) and total aortic diameter (35.5±6.0 vs. 39.9±8.1; p = 0.045). IVUS-guided stent graft sizing in Type B aortic dissection shows beneficial effects on aortic remodeling and might be of additional advantage in aortic diseases, especially when CT image quality is poor.
Conflict of interest statement
Figures
References
-
- Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014; 35: 2873–2926. doi: 10.1093/eurheartj/ehu281 - DOI - PubMed
-
- Hiratzka LF Invited commentary. Ann Thorac Surg. 2010; 90: 1521–1522. doi: 10.1016/j.athoracsur.2010.07.004 - DOI - PubMed
-
- Brunkwall J, Kasprzak P, Verhoeven E, Heijmen R, Taylor P, Trialists A, et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial. Eur J Vasc Endovasc Surg. 2014; 48: 285–291. doi: 10.1016/j.ejvs.2014.05.012 - DOI - PubMed
-
- Nienaber CA, Kische S, Rousseau H, Eggebrecht H, Rehders TC, Kundt G, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013; 6: 407–416. doi: 10.1161/CIRCINTERVENTIONS.113.000463 - DOI - PubMed
-
- Leshnower BG, Duwayri YM, Chen EP, Li C, Zehner CA, Binongo JN, et al. Aortic Remodeling After Endovascular Repair of Complicated Acute Type B Aortic Dissection. Ann Thorac Surg. 2017; 103: 1878–1885. doi: 10.1016/j.athoracsur.2016.09.057 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
