

A Trial of a Single-tablet Regimen of Elvitegravir, Cobicistat, Emtricitabine, and Tenofovir Disoproxil Fumarate for the Initial Treatment of Human Immunodeficiency Virus Type 2 Infection in a Resource-limited Setting: 48-Week Results From Senegal, West Africa
- PMID: 29672676
- PMCID: PMC6927863
- DOI: 10.1093/cid/ciy324
A Trial of a Single-tablet Regimen of Elvitegravir, Cobicistat, Emtricitabine, and Tenofovir Disoproxil Fumarate for the Initial Treatment of Human Immunodeficiency Virus Type 2 Infection in a Resource-limited Setting: 48-Week Results From Senegal, West Africa
Abstract
Background: There is an urgent need for safe and effective antiretroviral therapy (ART) for human immunodeficiency virus type 2 (HIV-2) infection. We undertook the first clinical trial of a single-tablet regimen containing elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate (E/C/F/TDF) to assess its effectiveness in HIV-2-infected individuals in Senegal, West Africa.
Methods: HIV-2-infected, ART-naive adults with World Health Organization stage 3-4 disease or CD4 count <750 cells/μL were eligible for this 48-week, open-label trial. We analyzed HIV-2 viral loads (VL), CD4 counts, clinical and adverse events, mortality, and loss to follow-up.
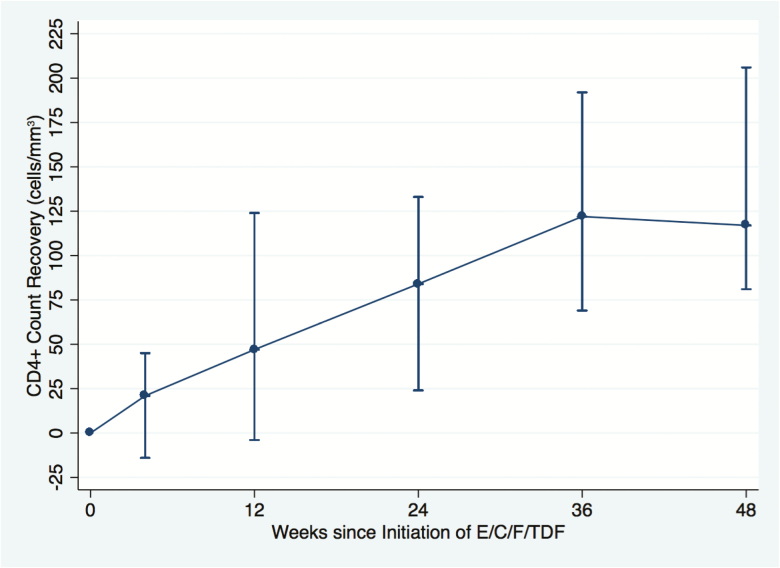
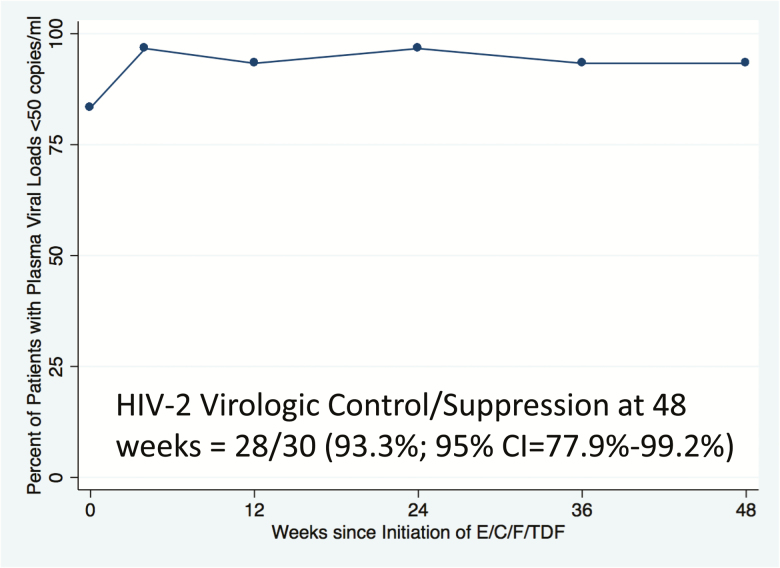
Results: We enrolled 30 subjects who initiated E/C/F/TDF. Twenty-nine subjects completed 48 weeks of follow-up. The majority were female (80%). There were no deaths, no new AIDS-associated clinical events, and 1 loss to follow-up. The median baseline CD4 count was 408 (range, 34-747) cells/μL, which increased by a median 161 (range, 27-547) cells/μL at week 48. Twenty-five subjects had baseline HIV-2 VL of <50 copies/mL of plasma. In those with detectable HIV-2 VL, the median was 41 (range, 10-6135) copies/mL. Using a modified intent-to-treat analysis (US Food and Drug Administration Snapshot method), 28 of 30 (93.3%; 95% confidence interval, 77.9%-99.2%) had viral suppression at 48 weeks. The 1 subject with virologic failure had multidrug-resistant HIV-2 (reverse transcriptase mutation: K65R; integrase mutations: G140S and Q148R) detected at week 48. There were 8 grade 3-4 adverse events; none were deemed study related. Adherence and acceptability were good.
Conclusions: Our data suggest that E/C/F/TDF, a once-daily, single-tablet-regimen, is safe, effective, and well tolerated. Our findings support the use of integrase inhibitor-based regimens for HIV-2 treatment.
Clinical trials registration: NCT02180438.
Figures
References
-
- De Cock KM, Adjorlolo G, Ekpini E et al. . Epidemiology and transmission of HIV-2. Why there is no HIV-2 pandemic [published erratum appears in JAMA 1994 Jan 19;271(3):196] [see comments]. JAMA 1993; 270:2083–6. - PubMed
-
- Joint United Nations Programme on HIV/AIDS. UNAIDS 2017. Available at: http://aidsinfo.unaids.org. Accessed 26 September 2017.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
