

Amaze: a randomized controlled trial of adjunct surgery for atrial fibrillation
- PMID: 29672731
- PMCID: PMC6134441
- DOI: 10.1093/ejcts/ezy165
Amaze: a randomized controlled trial of adjunct surgery for atrial fibrillation
Abstract
Objectives: Atrial fibrillation (AF) reduces survival and quality of life (QoL). It can be treated at the time of major cardiac surgery using ablation procedures ranging from simple pulmonary vein isolation to a full maze procedure. The aim of this study is to evaluate the impact of adjunct AF surgery as currently performed on sinus rhythm (SR) restoration, survival, QoL and cost-effectiveness.
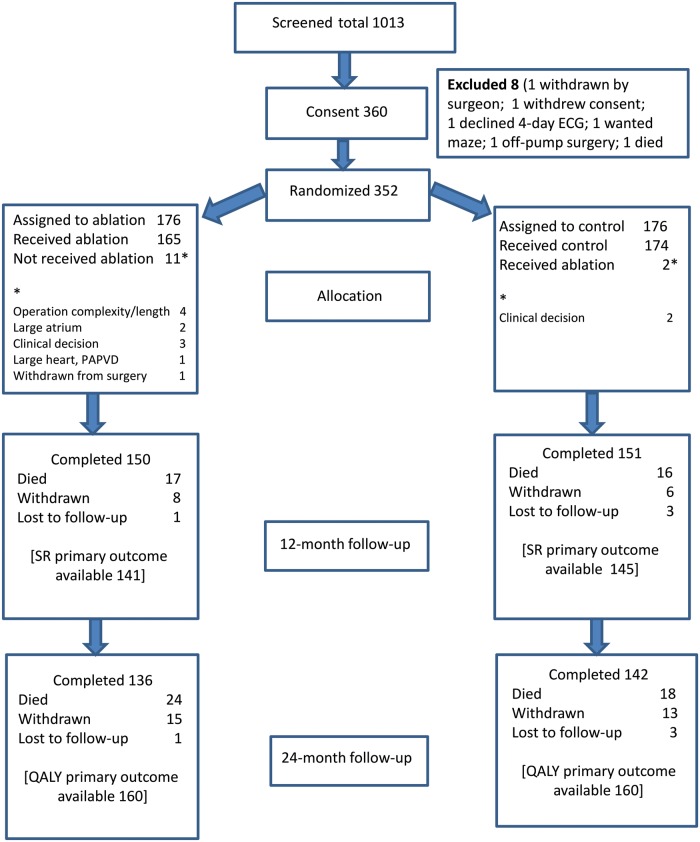
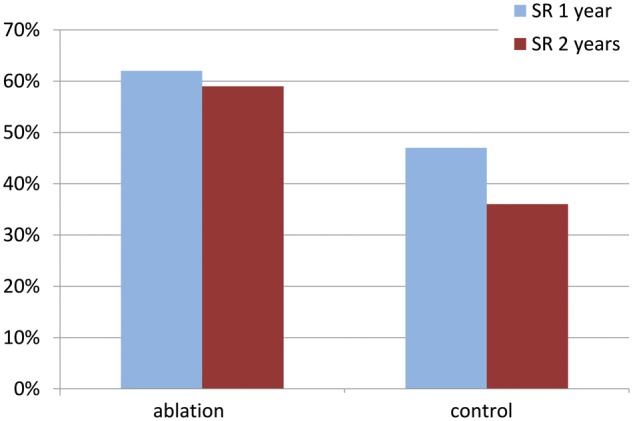
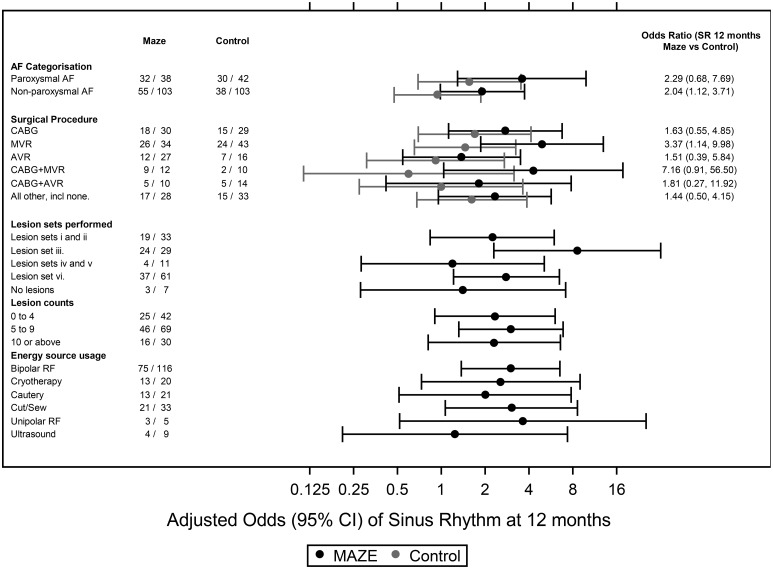
Methods: In a multicentre, Phase III, pragmatic, double-blinded, parallel-armed randomized controlled trial, 352 cardiac surgery patients with >3 months of documented AF were randomized to surgery with or without adjunct maze or similar AF ablation between 2009 and 2014. Primary outcomes were SR restoration at 1 year and quality-adjusted life years at 2 years. Secondary outcomes included SR at 2 years, overall and stroke-free survival, medication, QoL, cost-effectiveness and safety.
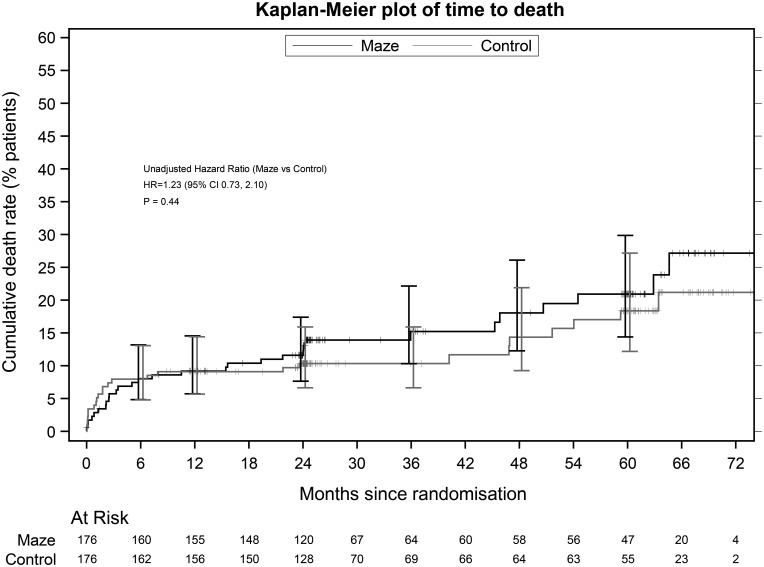
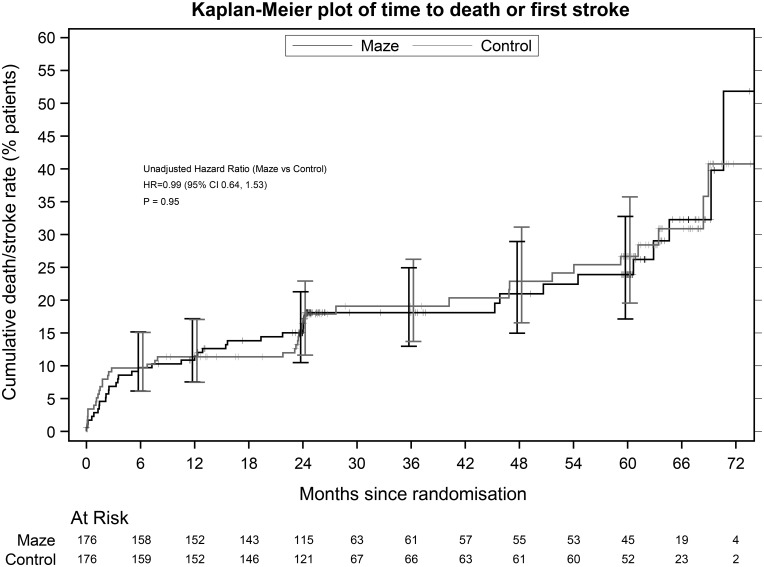
Results: More ablation patients were in SR at 1 year [odds ratio (OR) 2.06, 95% confidence interval (CI) 1.20-3.54; P = 0.009]. At 2 years, the OR increased to 3.24 (95% CI 1.76-5.96). Quality-adjusted life years were similar at 2 years (ablation - control -0.025, P = 0.6319). Significantly fewer ablation patients were anticoagulated from 6 months postoperatively. Stroke rates were 5.7% (ablation) and 9.1% (control) (P = 0.3083). There was no significant difference in stroke-free survival [hazard ratio (HR) = 0.99, 95% CI 0.64-1.53; P = 0.949] nor in serious adverse events, operative or overall survival, cardioversion, pacemaker implantation, New York Heart Association, EQ-5D-3L and SF-36. The mean additional ablation cost per patient was £3533 (95% CI £1321-£5746). Cost-effectiveness was not demonstrated at 2 years.
Conclusions: Adjunct AF surgery is safe and increases SR restoration and costs but not survival or QoL up to 2 years. A continued follow-up will provide information on these outcomes in the longer term.
Study registration: ISRCTN82731440 (project number 07/01/34).
Figures
References
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D.. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol 1998;82:2N–9N. - PubMed
-
- Hobbs FD, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S. et al. A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study. Health Technol Assess 2005;9:iii–v, ix–x, 1–74. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB.. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–8. - PubMed
-
- Friberg L, Rosenqvist M, Lip GY.. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J 2012;33:1500–10. - PubMed
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G. et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
