

Lenalidomide versus lenalidomide + dexamethasone prolonged treatment after second-line lenalidomide + dexamethasone induction in multiple myeloma
- PMID: 29673108
- PMCID: PMC6010717
- DOI: 10.1002/cam4.1422
Lenalidomide versus lenalidomide + dexamethasone prolonged treatment after second-line lenalidomide + dexamethasone induction in multiple myeloma
Abstract
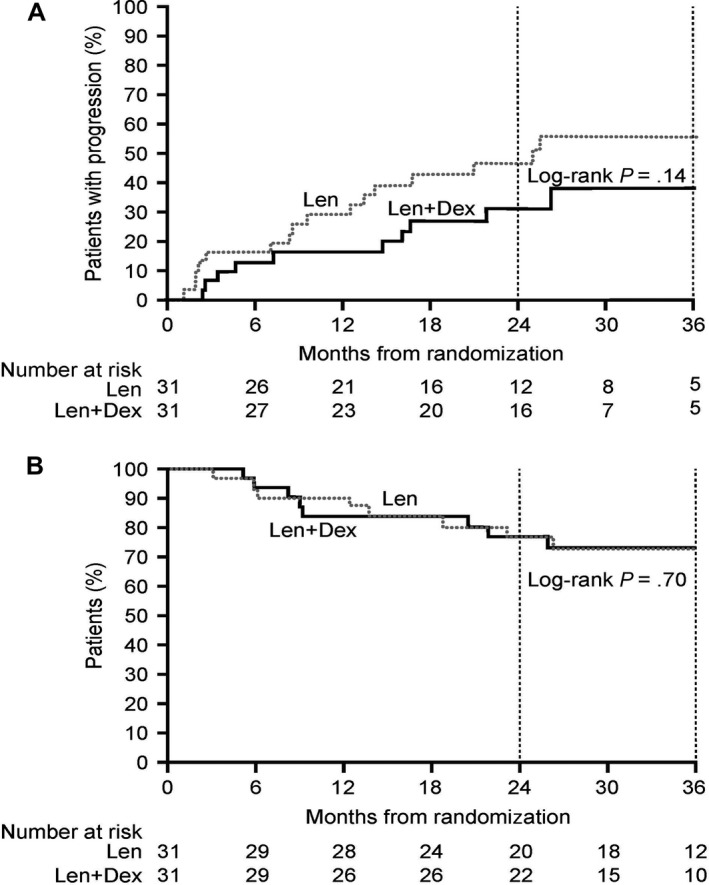
Lenalidomide (Len) plus dexamethasone (Dex) is approved for the treatment of relapsed or refractory multiple myeloma (RRMM). It is possible that single-agent Len may be effective as prolonged treatment regimen in RRMM once patients demonstrate an initial response to Len+Dex induction. Patients with RRMM who responded to first-line Len+Dex in an observational study (NCT01430546) received up to 24 cycles of either Len (25 mg/day) or Len+Dex (25 mg/day and 40 mg/week) as prolonged treatment in a subsequent phase 2 clinical trial (NCT01450215). In the observational study (N = 133), median time to response was 1.7 (range 0.6-9.6) months. A complete response to all treatments received in both studies was observed in 11% of patients; very good partial response and partial response rates were 31% and 38%, respectively. Corresponding response rates in the subgroup of patients who did not enter the phase 2 trial (n = 71) were 3%, 18%, and 39%, respectively. Rates of disease progression at 2 years in the phase 2 trial were 47% versus 31% for Len versus Len+Dex (P = 0.14). After 36 months median follow-up in surviving patients, median time to progression was not reached with Len+Dex and was 24.9 months (95% confidence interval 12.5-not calculable, P < 0.001) with Len. Three-year OS among the total observational study population was 61% (95% CI, 52-69%). The corresponding rate among patients who entered the phase 2 clinical trial was 73% (95% CI, 60-83%) and was significantly lower among those patients who achieved ≥PR but did not proceed into the phase 2 trial (55%; P = 0.01). In the phase 2 trial, OS was 73% in both treatment arms (P = 0.70). Neutropenia and thrombocytopenia were more common with prolonged (phase 2 trial) versus short-term (observational study) Len administration but remained manageable. Prolonged treatment with Len with or without Dex provides sustained, clinically relevant responses and demonstrates an acceptable safety profile.
Keywords: Clinical Trial; Lenalidomide; Multiple Myeloma.
© 2018 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures

References
-
- Liwing, J. , Uttervall K., Lund J., Aldrin A., Blimark C., Carlson K., et al. 2014. Improved survival in myeloma patients: starting to close in on the gap between elderly patients and a matched normal population. Br. J. Haematol. 164:684–693. - PubMed
-
- Lund, J. , Uttervall K., Liwing J., Gahrton G., Alici E., Aschan J., et al. 2014. Addition of thalidomide to melphalan and prednisone treatment prolongs survival in multiple myeloma – a retrospective population based study of 1162 patients. Eur. J. Haematol. 92:19–25. - PubMed
-
- McCormack, P. L. 2015. Lenalidomide: a review of its continuous use in patients with newly diagnosed multiple myeloma not eligible for stem‐cell transplantation. Drugs Aging 32:409–418. - PubMed
-
- Zagouri, F. , Terpos E., Kastritis E., and Dimopoulos M. A.. 2015. An update on the use of lenalidomide for the treatment of multiple myeloma. Expert Opin. Pharmacother. 16:1865–1877. - PubMed
-
- Celgene Corporation . REVLIMID prescribing information. 2015. Available at http://www.revlimid.com/wp-content/uploads/full-prescribing-information.pdf (accessed 1 November 2016).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
