

Benefits in pain perception, ability function and health-related quality of life in patients with failed back surgery syndrome undergoing spinal cord stimulation in a clinical practice setting
- PMID: 29673357
- PMCID: PMC5909225
- DOI: 10.1186/s12955-018-0887-x
Benefits in pain perception, ability function and health-related quality of life in patients with failed back surgery syndrome undergoing spinal cord stimulation in a clinical practice setting
Abstract
Background: Failed back surgery syndrome (FBSS) represents one main cause of chronic neuropathic or mixed pain, functional disability and reduced Health Related Quality of Life (HRQoL). Spinal Cord Stimulation (SCS) can be a value for money option to treat patients refractory to conventional medical management (CMM). We estimated from real-world data: 1) the amount of reduced levels of HRQoL of target patients compared to general population, 2) the relationship between pain intensity, functional disability, and overall HRQoL, and 3) the improvement of patients’ health from SCS intervention, and 4) we give some insights and make some suggestions on the selection of a battery of patients’ reported health instruments for use in routine clinical practice.
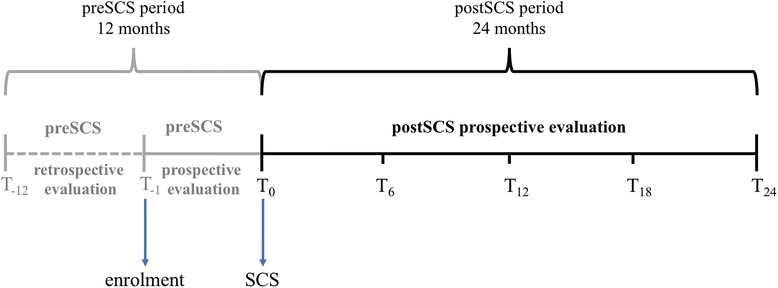
Methods: At recruitment (before SCS) and every 6 months for 2 years after SCS a battery of questionnaires/tests were completed: the generic EQ-5D and SF-36 for HRQoL, the specific Numerical Rating Scale (NRS) to measure pain intensity, and Oswestry Disability Index (ODI) to measure functional disability. We conducted multilevel regression analyses to investigate the association of HRQoL with the NRS and ODI indexes; multiple regression analyses to compare EQ-5D data with those of the general population adjusted for age, sex and education, and statistical tests to compare the changes of HRQoL, NRS and ODI estimates at baseline with those measured during the follow-up.
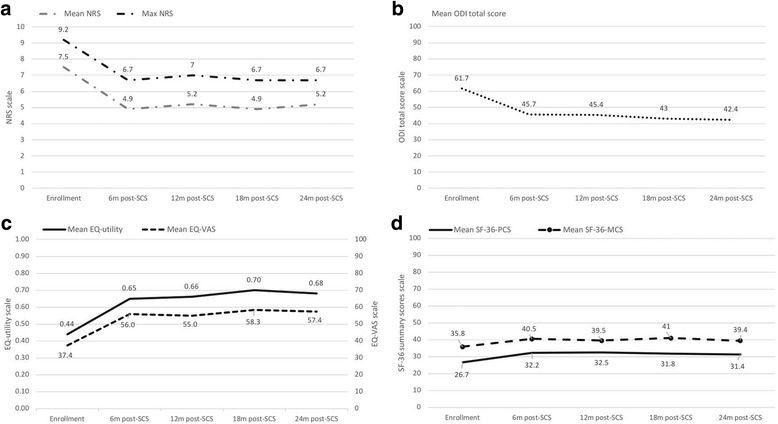
Results: Eighty patients (40% male, mean age = 58 years) participated. HRQoL was significantly worse in the patients than in the corresponding general population. Pain, functional disability and HRQoL significantly related each other during follow-up, Significant improvements (p < 0.001) in pain intensity, functional capability and HRQoL were reached after 6 months from SCS and generally remained stable during follow-up. Specific instruments provided detailed information on disability and pain, while generic instruments assessed the overall HRQoL and allowed a comparison with the general population’s one.
Conclusions: SCS + CMM treatment reaches a statistically significant and probably a clinically relevant improvement in pain perception, functional disability and HRQoL in patients with FBSS refractory to CMM. An appropriate selection of instruments for use in clinical practice is crucial for a routine assessment of health perception in patients, aimed to guide decisions for optimal treatment.
Background: Failed back surgery syndrome (FBSS) represents one main cause of chronic neuropathic or mixed pain, functional disability and reduced Health Related Quality of Life (HRQoL). Spinal Cord Stimulation (SCS) can be a value for money option to treat patients refractory to conventional medical management (CMM).
We estimated from real-world data: 1) the amount of reduced levels of HRQoL of target patients compared to general population, 2) the relationship between pain intensity, functional disability, and overall HRQoL, and 3) the improvement of patients’ health from SCS intervention, and 4) we give some insights and make some suggestions on the selection of a battery of patients’ reported health instruments for use in routine clinical practice.
Methods: At recruitment (before SCS) and every 6 months for 2 years after SCS a battery of questionnaires/tests were completed: the generic EQ-5D and SF-36 for HRQoL, the specific Numerical Rating Scale (NRS) to measure pain intensity, and Oswestry Disability Index (ODI) to measure functional disability. We conducted multilevel regression analyses to investigate the association of HRQoL with the NRS and ODI indexes; multiple regression analyses to compare EQ-5D data with those of the general population adjusted for age, sex and education, and statistical tests to compare the changes of HRQoL, NRS and ODI estimates at baseline with those measured during the follow-up.
Results: Eighty patients (40% male, mean age = 58 years) participated. HRQoL was significantly worse in the patients than in the corresponding general population. Pain, functional disability and HRQoL significantly related each other during follow-up, Significant improvements (p < 0.001) in pain intensity, functional capability and HRQoL were reached after 6 months from SCS and generally remained stable during follow-up. Specific instruments provided detailed information on disability and pain, while generic instruments assessed the overall HRQoL and allowed a comparison with the general population’s one.
Conclusions: SCS + CMM treatment reaches a statistically significant and probably a clinically relevant improvement in pain perception, functional disability and HRQoL in patients with FBSS refractory to CMM. An appropriate selection of instruments for use in clinical practice is crucial for a routine assessment of health perception in patients, aimed to guide decisions for optimal treatment.
Keywords: Disability; Failed back surgery syndrome; Health-related quality-of-life; Pain intensity; Spinal cord stimulation.
Conflict of interest statement
Ethics approval and consent to participate
The study participation of each center was previously approved by the Local Ethics Committee, present in each hospital according to the Italian regulations on clinical research. Eligible patients had to sign an informed consent form after receiving all the necessary information on the aim of the study, the type of data and the method of data collection.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Van Buyten JP, Linderoth B. The failed back surgery syndrome: definition and therapeutic algorithms – an update. Eur J Pain Supplements. 2010;4:273–286. doi: 10.1016/j.eujps.2010.09.006. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
