

P-Wave Amplitude and PR Changes in Patients With Inappropriate Sinus Tachycardia: Findings Supportive of a Central Mechanism
- PMID: 29674334
- PMCID: PMC6015284
- DOI: 10.1161/JAHA.118.008528
P-Wave Amplitude and PR Changes in Patients With Inappropriate Sinus Tachycardia: Findings Supportive of a Central Mechanism
Abstract
Background: The mechanism of inappropriate sinus tachycardia (IST) remains incompletely understood.
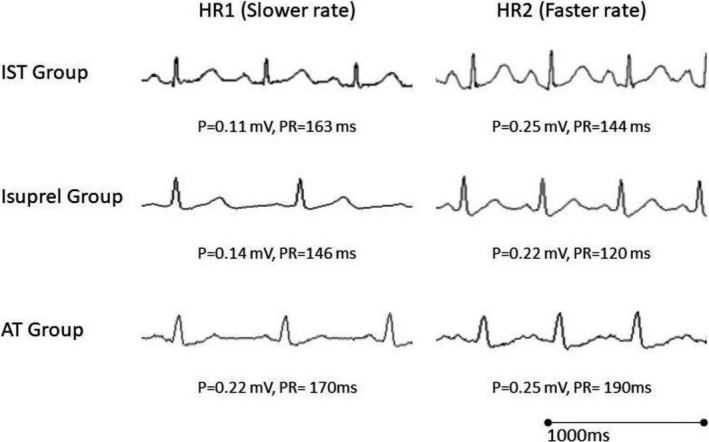
Methods and results: We prospectively compared 3 patient groups: 11 patients with IST (IST Group), 9 control patients administered isoproterenol (Isuprel Group), and 15 patients with cristae terminalis atrial tachycardia (AT Group). P-wave amplitude in lead II and PR interval were measured at a lower and higher heart rate (HR1 and HR2, respectively). P-wave amplitude increased significantly with the increase in HR in the IST Group (0.16±0.07 mV at HR1=97±12 beats per minute versus 0.21±0.08 mV at HR2=135±21 beats per minute, P=0.001). The average increase in P-wave amplitude in the IST Group was similar to the Isuprel Group (P=0.26). PR interval significantly shortened with the increases in HR in the IST Group (146±15 ms at HR1 versus 128±16 ms at HR2, P<0.001). A similar decrease in the PR interval was noted in the Isuprel Group (P=0.6). In contrast, patients in the atrial tachycardia Group experienced PR lengthening during atrial tachycardia when compared with baseline normal sinus rhythm (153±25 ms at HR1=78±17 beats per minute versus 179±29 ms at HR2=140±28 beats per minute, P<0.01).
Conclusions: We have shown that HR increases in patients with IST were associated with an increase in P-wave amplitude in lead II and PR shortening similar to what is seen in healthy controls following isoproterenol infusion. The increase in P-wave amplitude and absence of PR lengthening in IST support an extrinsic mechanism consistent with a state of sympatho-excitation with cephalic shift in sinus node activation and enhanced atrioventricular nodal conduction.
Keywords: atrial tachycardia; atrio‐ventricular conduction; inappropriate sinus tachycardia.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Sheldon RS, Grubb BP II, Olshansky B, Shen WK, Calkins H, Brignole M, Raj SR, Krahn AD, Morillo CA, Stewart JM, Sutton R, Sandroni P, Friday KJ, Hachul DT, Cohen MI, Lau DH, Mayuga KA, Moak JP, Sandhu RK, Kanjwal K. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12:e41–e63. - PMC - PubMed
-
- Olshansky B, Sullivan RM. Inappropriate sinus tachycardia. J Am Coll Cardiol. 2013;61:793–801. - PubMed
-
- Pellegrini CN, Scheinman MM. Epidemiology and definition of inappropriate sinus tachycardia. J Interv Card Electrophysiol. 2016;46:29–32. DOI: 10.1007/s10840‐015‐0039‐8. - DOI - PubMed
-
- Lee RJ, Shinbane JS. Inappropriate sinus tachycardia. Diagnosis and treatment. Cardiol Clin. 1997;15:599–605. - PubMed
-
- Segerson NM, Wasmund SL, Daccarett M, Fabela ML, Hammond CH, Stoddard G, Smith ML, Hamdan MH. The acute effect of atrioventricular pacing on sympathetic nerve activity in patients with normal and depressed left ventricular function. Am J Physiol Heart Circ Physiol. 2008;295:H1076–H1080. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
